
Professor Yuping Wang – Vitamin D and Preeclampsia – Joining the Dots
Preeclampsia is a common but serious complication of pregnancy that can harm both mother and baby. Recent research has identified vitamin D deficiency as a risk factor for developing preeclampsia and also the beneficial effects of vitamin D supplementation on this pregnancy disorder, but the mechanisms for this are still not clear. Professor Yuping Wang at Louisiana State University has been investigating this question by studying the effects of vitamin D on the placenta.
The Global Problem of Preeclampsia
Pregnancy and birth are getting safer every decade – however, preeclampsia, a disorder of pregnancy characterised by the onset of high blood pressure and often a significant amount of protein in the urine, is still one of the most common serious complications. Around one in 20 pregnant women will experience symptoms of the condition, increasing the risk of harm to both mother and baby. Preeclampsia is also a recognised risk factor for cardiovascular diseases in women later in life.
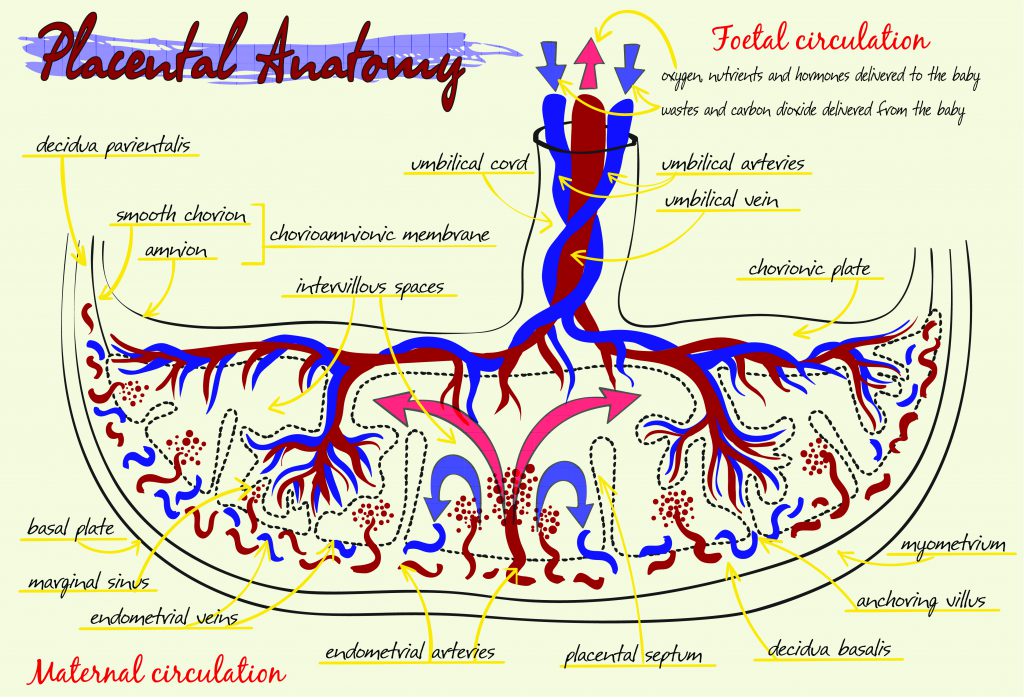
For the developing foetus in the womb the placenta is the doorway that allows access to the necessities of life. In this disc-shaped organ, foetal blood passes close enough to the mother’s blood so that a life-giving exchange is able to take place. The foetus receives oxygen in exchange for carbon dioxide and nutrients in exchange for waste.
In preeclampsia this essential process is disrupted as the mother’s uterine blood vessels do not adapt to pregnancy as they should and are unable to supply the placenta with enough blood. Unfortunately, although some risk factors have been identified, and symptomatic treatments are available, there is still much that is not known about what causes preeclampsia and how to stop it.
Further research is essential if this common, but dangerous, condition is to be consigned to the history books. One of those leading the charge is Professor Yuping Wang at Louisiana State University. With a career in placental research spanning almost 30 years, she is now focusing on a recently identified risk factor for developing preeclampsia – vitamin D deficiency – and has been investigating in detail the actions of vitamin D on the placenta.
‘We propose that normalisation of vitamin D receptor function to improve vitamin D responsiveness in placental trophoblasts during preeclampsia may correct and restore trophoblast function that would lead to a decrease in severity and reduce the incidence of preeclampsia.’
The Placenta – ‘The Tree of Life’
The structure of the placenta is uniquely adapted for its function. It contains spaces in which maternal blood pools, ready for the exchange of gases and nutrients to take place. Finger-like projections, termed villi, branch out from the foetal side and extend into these pools. These villi contain blood vessels from the embryo (foetus) at their core, and their surface is covered with a specialised type of cell called trophoblasts.
The tree-like structure of the villi in the placenta creates a surface area of around 12 square metres for the exchange of oxygen, carbon dioxide and nutrients. Towards the end of pregnancy, this forest of villi contains approximately 320 kilometres of foetal blood vessels – that’s enough to stretch from Dover in England, to Calais in France, and back five times.
E-book
Audio-book
Reference
https://doi.org/10.26320/SCIENTIA143
Share
{kind=link}
Maternal and foetal blood do not mix in the placenta – instead, the exchange takes place through diffusion, with the trophoblasts providing an important biochemical and physical barrier between the two sides.
 These specialised cells also produce numerous hormones and growth factors that are required for and can influence the development of the placenta and the foetus. These include vascular endothelial growth factor (VEGF) family molecules such as placental growth factor (PlGF) and vasoactivators such as thromboxane and prostacyclin, which can regulate placental blood vessel development and function, respectively. Some trophoblasts migrate to the maternal uterine blood vessels during the development of the placenta to promote uterine blood vessel adaptation to pregnancy and increase maternal blood flow into the placenta.
These specialised cells also produce numerous hormones and growth factors that are required for and can influence the development of the placenta and the foetus. These include vascular endothelial growth factor (VEGF) family molecules such as placental growth factor (PlGF) and vasoactivators such as thromboxane and prostacyclin, which can regulate placental blood vessel development and function, respectively. Some trophoblasts migrate to the maternal uterine blood vessels during the development of the placenta to promote uterine blood vessel adaptation to pregnancy and increase maternal blood flow into the placenta.
In preeclampsia, these trophoblasts don’t appear to travel as far along the maternal blood vessels as they should, resulting in reduced blood flow into the placenta. This results in decreased oxygen delivery to the trophoblast tissue, inducing a state of hypoxia (oxygen deprivation), which has a knock-on effect on many cellular processes.
Hypoxia induces a state of oxidative stress in these cells, characterised by the increased production of reactive oxygen species (ROS), inflammatory cytokines, and vasoconstrictors, which can enter the maternal blood stream and induce maternal vascular dysfunction in preeclampsia. Professor Wang is clear that these changes are not inconsequential: ‘placental trophoblast dysfunction plays a central role in the pathogenesis of preeclampsia,’ she says, so it’s essential that we understand why and how.
Vitamin D and the Cells of the Placenta
Could vitamin D hold the key to answering those questions? Professor Wang and her team think it might and have published multiple pieces of research over the past five years that point in that direction. It is known that not having enough vitamin D during pregnancy increases the risk of developing preeclampsia, but how vitamin D is able to affect events in the placenta is less clear.
The first question Professor Wang and her team asked was whether the trophoblasts of the placenta have the ability to produce or respond to vitamin D. Vitamin D can be absorbed from food or it can be produced in the body after the skin is exposed to sunlight. The active form of vitamin D is formed from a precursor molecule that is modified by several enzymes present in certain cell types and is then secreted from those cells. This active form of vitamin D then binds to receptors on its target cells to induce a response in them.
Professor Wang and the team looked for the presence of these vitamin D enzymes and receptors in placental trophoblasts. They found that trophoblasts in the placenta are capable of both secreting, and responding to vitamin D. On top of that, cells from preeclamptic placentas had altered levels of these enzymes, along with reduced amounts of the vitamin D receptor, linking the state of preeclampsia with changes in the regulation of the vitamin D system in trophoblast cells.
Similarly, they found that in cells from the umbilical cord, mimicking preeclampsia by inducing hypoxia and oxidative stress in the laboratory, led to decreased levels of the vitamin D receptor and the natural antioxidant CuZn-SOD. Antioxidants like CuZn-SOD usually counteract the effects of oxidative stress by removing harmful superoxides from the cell.
Both the vitamin D receptor and CuZn-SOD levels could be returned to normal by applying vitamin D to the cells. This is an important finding, as it suggests that vitamin D can act at the cellular and molecular level in the placenta to reverse the effects of oxidative stress in these cells.
Next, the team asked whether vitamin D could reverse any of the alterations to trophoblast function observed in preeclampsia. One such alteration is an oxidative stress-induced increase in the production of thromboxane, a potent vasoconstrictor that promotes contraction of blood vessels. Professor Wang found that the application of vitamin D to placental cells was able to reduce this increased thromboxane production.
This suggests that in the placenta, vitamin D could correct the ratio of vasoconstrictor thromboxane and vasodilator prostacyclin production through its action on trophoblasts, increasing blood flow into the placenta, correcting the oxygen deprived state induced by vasoconstriction in placental vasculature in preeclampsia.
Following this, Professor Wang turned her attention to the muscle cells of the placental vessels themselves that allow them to change shape altering blood flow. She found that in placental vascular smooth muscle cells, applying vitamin D could not only upregulate the expression of the vitamin D receptor but can also reduce angiotensin II – another potent vasoconstrictor – induced contraction of the smooth muscle cells of placental blood vessels.
This suggests that, like the placental trophoblasts, the muscle cells lining the blood vessel are able to respond to vitamin D. It also suggests a feedback system in which cells respond to increased vitamin D levels by reducing their own production. Interestingly, vitamin D was able to induce relaxation of blood vessel muscle cells in the laboratory. Professor Wang and her team also identified a potential molecular mechanism of vitamin D to relax muscle cells of placental blood vessels, similar to that of losartan, an angiotensin II receptor 1 (AT1) blocker, by inducing a signalling mechanism called phosphorylation of the myosin phosphatase target subunit 1 (MYPT1) pathway molecule. This is the key player involved in myosin light chain phosphatase (MLCP) activation that is essential for vessel dilation or relaxation.
In preeclamptic placentas, trophoblasts enter a state of oxidative stress and increase the number of micro-particles they release into the maternal bloodstream. These micro-particles induce an inflammatory response and affect maternal adaptation to pregnancy that can contribute to the abnormal changes in maternal vasculature and immune systems seen in preeclampsia.
In her most recent work, Professor Wang found that, when preeclampsia is mimicked in these cells in the laboratory by reducing oxygen levels, it is possible to measure an increase in the generation of superoxides and micro-particle release. When vitamin D was applied to these cells, both of these measures were then reduced.
Taken together, these findings join some of the dots between vitamin D deficiency and preeclampsia risk, and the molecular and cellular events taking place in the placenta itself. They paint a picture of vitamin D as an anti-oxidative and anti-inflammatory molecule that can act on placental trophoblasts and endothelial cells to reduce the changes in function that occur in these cells in preeclampsia.
Vitamin D can also cause the relaxation of blood vessel muscle cells to increase blood flow and could reduce the oxygen deprivation seen in preeclamptic placentas that is potentially harmful to the baby.

Future Directions
The big picture goal of Professor Wang’s research is to make pregnancy safer, so how does she plan to apply this new knowledge about the role of vitamin D to clinical practice? It’s not just about popping some vitamin D supplements when you’re expecting.
Her finding that there are reduced amounts of the vitamin D receptor on trophoblasts in preeclampsia suggests that these cells may not be able to respond correctly to vitamin D, even if it is there.
Her solution? To find a way of upregulating vitamin D receptor production during preeclampsia specifically in trophoblast cells, with the aim of restoring normal trophoblast function and decreasing the severity of the condition.
She describes how, ‘we propose that normalisation of vitamin D receptor function to improve vitamin D responsiveness in placental trophoblasts during preeclampsia may correct and restore trophoblast function that would lead to a decrease in severity and reduce the incidence of preeclampsia.’ The team is exploring this exciting new possibility and the next few years of Professor Wang’s work will be focused on bringing them closer to this goal.
Meet the researcher

Professor Yuping Wang
Department of Obstetrics and Gynaecology
Department of Cellular and Molecular Physiology
Louisiana State University Health Sciences Centre
Shreveport, LA
USA
Professor Yuping Wang is a tenured professor in the department of Obstetrics and Gynaecology and the department of Cellular and Molecular Physiology at Louisiana State University Health Sciences Centre, Shreveport, USA. She received her MD from Harbin Medical University, China, in 1980 and her PhD from the Medical College of Virginia at Virginia Commonwealth University, USA, in 1994. Professor Wang currently serves on the editorial board of the International Journal of Reproductive Medicine and the Journal of Nephrology Research. Her major area of research is placental trophoblast and vascular endothelial function in pregnancy, including in pregnancy complications such as preeclampsia.
CONTACT
E: YWang1@lsuhsc.edu
T: (+1) 318-675-5379
W: https://www.shreveportphysiology.com/faculty/emeritus-adjunct-faculty/
FUNDING
National Institutes of Health, Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD)
FURTHER READING
J Xu, X Jia, Y Gu, DF Lewis, X Gu and Y Wang, 1,25(OH)2D3 reduces oxidative stress-induced procaspase-3/ROCK1 activation and MP release by placental trophoblasts, Journal of Clinical Endocrinology and Metabolism, 2017, 102, 2100–2110.
X Jia, J Xu, Y Gu, X Gu, W Li and Y Wang, Vitamin D suppresses oxidative stress-induced microparticle release by human umbilical vein endothelial cells, Biology of Reproduction, 2017, 96, 199–210.
X Jia, Y Gu, LJ Groome, M Al-kofahi, JS Alexander, W Li and Y Wang, 1,25(OH)2D3 induces placental vascular smooth muscle cell relaxation by phosphorylation of myosin phosphatase target subunit 1Ser507: Potential beneficial effects of vitamin D on placental vasculature in humans, Biology of Reproduction, 2016, 94, 116, 1–8.
J Sun, W Zhong, Y Gu, LJ Groome and Y Wang, 1,25(OH)2D3 suppresses oxidative stress-induced COX-2 up-regulation and thromboxane production by placental trophoblast cells, Placenta, 2014, 35, 2, 143-5.
W Zhong, B Gu, Y Gu, LJ Groome, J Sun and Y Wang, Activation of vitamin D receptor promotes VEGF and CuZn-SOD expression in endothelial cells, Journal of Steroid Biochemistry Molecular Biology, 2014, 140, 56–62.
R Ma, Y Gu, S Zhao, J Sun, LJ Groome and Y Wang, Expressions of vitamin D metabolic component VDBP, CYP2R1, CYP27B1, CYP24A1, and VDR in placentas from normal and preeclamptic pregnancies, American Journal of Physiology – Endocrinology and Metabolism, 2012, 303, E928–35.
![]()