
Dr Sharon Brennan-Olsen – The Social Gradient in Musculoskeletal Health
Disease is as much a social and economic phenomenon as a biological one. Dr Sharon Brennan-Olsen and her team at the University of Melbourne, and the Australian Institute for Musculoskeletal Science (AIMSS), are investigating musculoskeletal disorders as a socioeconomic-related health outcome.
The Social Determinants of Musculoskeletal Disorders
Health and disease are shaped not only by biology but also by several social, demographic, economic, policy and behavioural factors – the ‘social determinants of health’. Numerous analyses attest to the associations between socioeconomic indicators and health outcomes. It is well-documented that socially disadvantaged populations have worse health outcomes than their privileged counterparts – a phenomenon termed the ‘social gradient of health’. Indeed, many physical diseases and poorer health outcomes are observed to disproportionately affect disadvantaged and marginalised people, including– as we shall see – musculoskeletal disorders. While this may often be attributed to ‘poverty’, the reality is far more complex, and the social gradient is indicative of deep social and economic inequalities. As well as having low economic capital, poorer individuals may have lower social capital, less extensive social networks with fewer support mechanisms, fewer choices, and often limited access to, or understanding about, health care services – factors that negatively influence health outcomes.
The skeleton, together with muscle, cartilage, tendons, ligaments, joints and other connective tissues, constitutes the musculoskeletal system. This forms a robust internal framework that provides support, stability and movement to the body – although there is plenty of scope for damage or ‘insult’ to the musculoskeletal system. Musculoskeletal disorders (MSDs), such as arthritis, osteoporosis, sarcopenia, osteosarcopenia, musculoskeletal trauma and injury can be extremely debilitating. These disorders can all result in a reduced quality of life and increased dependence on others. As such, they can severely affect an individual’s life and make everyday activities that most of us take for granted – walking the dog, grocery shopping, making the bed, lifting objects – extremely difficult. In addition, the prevalence of MSDs can impose significant personal burden, and dramatically increase the economic burden on healthcare systems. MSDs can also result in earlier mortality. Unsurprisingly, the social gradient in health is strongly represented in musculoskeletal disease.
Dr Sharon Lee Brennan-Olsen of the University of Melbourne and the Australian Institute for Musculoskeletal Science (AIMSS) is interested in understanding the social determinants of MSDs and related health service utilisation. ‘My program of research focuses on understanding why the social gradient exists and identifying potential points for intervention, including underlying biological factors such as inflammation,’ she says.
The Social Gradient of Arthritis
Arthritis is an umbrella term for more than 100 chronic, painful, debilitating diseases that most often affect joints. The most common forms are osteoarthritis and rheumatoid arthritis. Osteoarthritis is characterised by progressive degeneration of joint cartilage and swollen joints, mainly affecting the fingers, knees, and hips, amongst other joints. Rheumatoid arthritis is an autoimmune disorder that results in systemic inflammation of the joints, and subsequently influences many of the body’s systems.
Worldwide, arthritis affects one in four adults: 43% of those will have activity limitations due to their arthritis. Arthritis is not contained only to those living in higher-income countries. Rather, it presents a particularly complex problem for residents of lower- and middle-income countries – countries that have 90% of the global burden of arthritis, but only 12% of global health spending. For those with arthritis in lower- and middle-income countries, the disease imposes a vicious cycle that may act to worsen poverty, as they often have poor access to health and social services, reduced employment opportunities and pension options, and fewer social security ‘safety nets’ than those in higher-income countries.
Download
Listen
Reference
https://doi.org/10.26320/SCIENTIA24
Share
{kind=link}

The World Health Organization (WHO) has compiled longitudinal data from over 44,000 respondents aged 50 years and older in six lower- and middle-income countries: China, Ghana, India, Mexico, Russian Federation and South Africa. Dr Brennan-Olsen and colleagues stratified respondent data from the WHO’s study on global AGEing and adult health (SAGE) by age, sex and socioeconomic factors, providing insight on the association between these factors and arthritis prevalence in lower- and middle-income countries. In the entire study population, for men and women respectively, they found that 20% and 14% had self-reported (lifetime) arthritis, while 5% and 3% had current symptom-based arthritis. The team also found that, similar to higher-income countries, arthritis prevalence increased proportionally with age. For both sexes and in all the countries studied, the researchers found that arthritis was more prevalent among those with the least education, and in women who were separated, divorced or widowed. After age-standardisation, men in five of the six countries were twice as likely as women to have arthritis, and in Ghana, men were three times as likely. The highest rates of arthritis were observed in Russia, in 38% of men and 17% of women.
These findings have important implications for resource-poor countries. The high prevalence of arthritis observed in lower- and middle-income countries emphasise the need for health authorities to direct resources towards arthritis prevention and treatment. Moreover, individuals living in poverty and with a low level of education may be predisposed to arthritis onset, as they are more likely to be employed as manual labourers. Dr Brennan-Olsen and her team are now investigating occupation types and occupational-related physical exposures as risk factors for arthritis.
Residents of higher-income countries are not immune to the impact of social and economic burdens on MSDs such as arthritis: just as in poorer countries, arthritis disproportionately affects those who are socioeconomically disadvantaged. Dr Brennan-Olsen and her colleagues investigated the social gradient of surgery related to osteoarthritis in her own country of Australia, by examining the association between socioeconomic status and uptake of total knee joint replacement (TKR). By analysing patient demographic data from the Australian Orthopaedic Association National Joint Replacement Registry, they found that there was a negative relationship between socioeconomic status and TKR uptake, with both men and women in the lowest 10% of socioeconomic status consistently more likely to undergo TKR than those in the highest 10%.
While these results are reflective of the well-documented social health gradient, the reality may be more complex. Individuals with lower socioeconomic status may wait in pain for longer than their less disadvantaged counterparts, most often due to having fewer economic resources on which to draw, less social support to rely upon during the necessary recovery period, and a reduced ability to take time away from work (if employed). Furthermore, individuals of lower socioeconomic status typically have a lower health literacy, which means they are less likely to seek, access, understand and implement health-related information. Patients with a higher socioeconomic status may also have greater financial resources and flexibility to access other modes of osteoarthritis management, such as private healthcare, physiotherapy, analgesics and early retirement.

The Social Gradient of Osteoporosis and Fractures
Bones are metabolically active organs, and undergo continuous remodelling across the lifespan, whereby mature bone tissue is removed (called resorption) and new bone tissue is formed (called formation). The remodelling process is both systemic and local – disturbances in this remodelling process can lead to deterioration of the bone matrix and a progressive decrease in bone mineral density, leading to increased risk of osteoporosis. Osteoporosis is the most common of the bone diseases: worldwide, osteoporosis affects 1 in 3 women and 1 in 5 men over the age of 50 years.
In recent years, there has been increasing interest in elucidating associations between socioeconomic disadvantage and low bone mineral density, and the subsequent risk of osteoporosis. Dr Brennan-Olsen and her colleagues recently used demographic data from patient records in Canada to examine the association between income and bone mineral density in more than 50,000 women aged 50 years and older. They found that there was a strong dose-response association between low income and low bone density, independent of known clinical risk factors. Women at the lowest income quintile were found to be 40% more likely to have low bone density (at the hip) than those at the highest income quintile – suggesting the existence of a social gradient in osteoporosis risk. Lower uptake of regular physical activity, lower dietary calcium intake, and a greater prevalence of smoking are all low income-related factors that may possibly contribute to this lower bone mineral density.
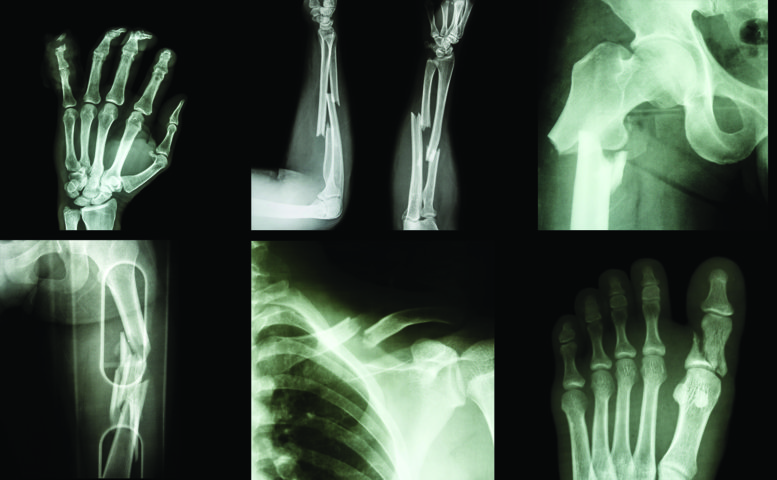
Bone fractures can happen due to high force impact or stress, such as playing football or rugby. But in patients with bone-weakening diseases such as osteoporosis, even minimal impact – for instance a fall from standing height or less – can result in fractures. Worldwide, an osteoporotic fracture is estimated by the International Osteoporosis Foundation to occur every 3 seconds.
Whether due to bone-weakening diseases or not, fractures can be financially, personally and psychosocially disastrous for individuals. They are more prevalent in the elderly, with higher incidence in women than men. However, fractures can happen to anyone, at any age and for many reasons. Nevertheless, the social gradient of health outcomes also appears to apply to fractures – and Dr Brennan-Olsen and her team have extensively studied this. They found that in Australians aged 50 years and over, disadvantaged men and women have increased fracture incidence compared to their less disadvantaged counterparts, represented by a six-fold and two-fold greater odds, respectively. The apparent disparity, not only across socioeconomic status but also sex, warrants further investigation.
Worldwide, indigenous populations experience disproportionally poorer health outcomes, greater morbidity and reduced life expectancy than their non-indigenous counterparts. Dr Brennan-Olsen and her team reviewed fracture rates in indigenous and non-indigenous populations, in a project that involved sifting through more than 3000 published articles containing real-world fracture data in PubMed, OVID, CINAHL and EMBASE databases. The only countries for which data were available were Australia, Mexico, USA and New Zealand. The findings of this study – thought to be the first of its kind – have been incredibly insightful.
The team found a greater incidence of trauma-related facial fractures in indigenous persons compared to non-indigenous persons. Compared to their non-indigenous counterparts, Canadian First Nations people had an almost five-fold greater risk of craniofacial fractures, New Zealand Maori people had an almost three-fold greater risk of facial fractures respectively, and Australian indigenous men had an almost eight-fold greater risk of jaw fractures. However, most shockingly, jaw fractures were 22-times greater in Australian indigenous women compared to non-indigenous Australian women. For hip fractures, however, the researchers found that indigenous people were at lower risk than their non-indigenous counterparts in all countries – with the exception of Canada and Australia where the opposite was observed.
This review also identified the risk factors associated with fractures that are disproportionately experienced by indigenous persons – comorbid diseases such as diabetes, and risk-taking behaviours such as substance abuse, and the reality that indigenous persons were more often victims of trauma resulting in fractures (for instance traffic accidents and interpersonal violence) compared to non-indigenous persons. This study provides insight into deep socioeconomic inequalities between indigenous and non-indigenous communities, and emphasises the priority of governments, global health initiatives, communities – and indeed wider society – to strive for equality for all.
Future Directions for Musculoskeletal Health
Dr Brennan-Olsen and her team are committed to investigating MSDs, as an outcome strongly related to social and economic disparities within lower-, middle- and higher-income societies across the world. Through their real-world observational studies, they demonstrate that musculoskeletal health is no exception to the observed social gradient in health: this gradient can be observed in all countries spanning the economic development continuum. Dr Brennan-Olsen’s more recent studies have focused on underpinning the biological mechanisms that underpin the social gradient of MSDs – especially biomarkers such as inflammation and epigenetic mechanisms.
Methylation of DNA influences the phenotypic expression of disease via a range of physiological processes – including bone development. A number of recent studies suggest that socially-related environmental factors can influence DNA methylation – providing a potential epigenetic explanation for the social gradient in musculoskeletal health. Dr Brennan Olsen, her team and colleagues have proposed a conceptual model that describes how social and environmental stressors – starting in utero, and occurring during early life, adolescence and adulthood – influence DNA methylation, which they hypothesise leads to inflammatory dysregulation and thus an increased risk of osteoporotic fracture.
In another future research direction, the team is investigating the social determinants of sarcopenia, a disease characterised by loss of muscle and loss of strength, and only added to the International Classification of Diseases in 2016. Combined with the presence of osteoporosis, both diseases together result in a condition referred to as osteosarcopenia. ‘Osteosarcopenia, an even less understood condition than sarcopenia, is also taking priority in my program of population health research,’ states Dr Brennan-Olsen.
Meet the researcher

Dr Sharon Lee Brennan-Olsen
The University of Melbourne
Department of Medicine-Western Health
Australian Institute for Musculoskeletal Science (AIMSS)
Melbourne
Australia
Dr Sharon Brennan-Olsen gained her PhD in the Department of Epidemiology and Preventive Medicine, Monash University, Australia in 2010. She has since completed a number of Fellowships and research appointments, before starting her current position as Senior Research Fellow with the Department of Medicine-Western Health, University of Melbourne, and Program Director of ‘Population Health-Musculoskeletal Disease’ at the Australian Institute for Musculoskeletal Science (AIMSS). Her research interests are the social determinants of musculoskeletal diseases and related health service utilisation, and her more recent investigations have focused on biological mechanisms, such as inflammatory biomarkers and epigenetic processes, that she has posited may underpin the social gradient of osteoporosis, sarcopenia, osteosarcopenia and arthritis diseases. She is also committed to knowledge translation of research findings to healthcare professionals, policy makers and the general population, particularly disadvantaged communities. Her many outreach efforts include managing the Osteosarcopenia Roadshow (an accredited training workshop for General Practitioners), holding a position on the Women in Bone and Mineral Science Committee for the American Society for Bone and Mineral Research, promoting osteoporosis awareness on ‘World Osteoporosis Day’ and during ‘Healthy Bones Week’.
CONTACT
E: sbrennan@unimelb.edu.au
T: (+61) 8395 8114
W: http://findanexpert.unimelb.edu.au/display/person125267
W: aimss.org.au
twitter: @Brennan_Olsen
FUNDING (current and previous)
National Health and Medical Research Council (NHMRC) of Australia: Career Development Fellowship (current), and an Early Career Researcher and Postgraduate Scholarship (both previous)
Arthritis Australia (Zimmer Australia)
Arthritis Victoria
Victorian Orthopaedic Research Trust
Australian Association of Gerontology
City of Greater Geelong
The University of Melbourne
Deakin University
![]()
![]()