
James J. Driscoll, MD, PhD | Immunoproteasome Activation Enhances the Recognition of Tumour Cells and Boosts Anticancer Immune Responses
Article written by Chris Barton, BSc (Hons), MSc (Hons)
The correct functioning of the human immune system depends on its ability to recognise danger, such as tumour cells, viruses, and bacteria. Scientists are learning how immunoproteasome activation can overcome the mechanisms by which cancer cells escape immune responses. Immunoproteasomes are small high molecular weight protein-degrading machines that signpost abnormal proteins made by cancer cells, directing the immune system against them. Dr James Driscoll at University Hospitals Cleveland Medical Center is using novel proprietary small molecules to selectively boost the catalytic activity of immunoproteasomes, which increases the tumour killing (or cytotoxic) effect of a group of white cells called T-cells. These findings provide a strong rationale for developing personalised therapeutics that target immunoproteasomes, for cancer and other immune-mediated conditions.
Multiple myeloma is a type of blood cancer that starts in a group of identical plasma cells, which then expand to form an increasing large population in the body. Myeloma cells are able to hide from the immune system, and hence resist treatments that use the body’s own defences. These treatments include immunomodulatory drugs (IMiDs) and monoclonal antibodies that prevent tumour cells from using natural pauses in immune cell activity to hide.
While such T-cell therapies have worked well in some cancers, multiple myeloma often escapes detection. It does this by switching off key parts of the system that normally help the immune system in spotting cancer — including natural proteins that flag tumour cells to killer immune cells. These different proteins often arise from cancer-specific genetic mutations, abnormal RNA processing, or changes in how proteins are modified.
The Role of Proteasomes and Immunoproteasomes in Antigen Presentation
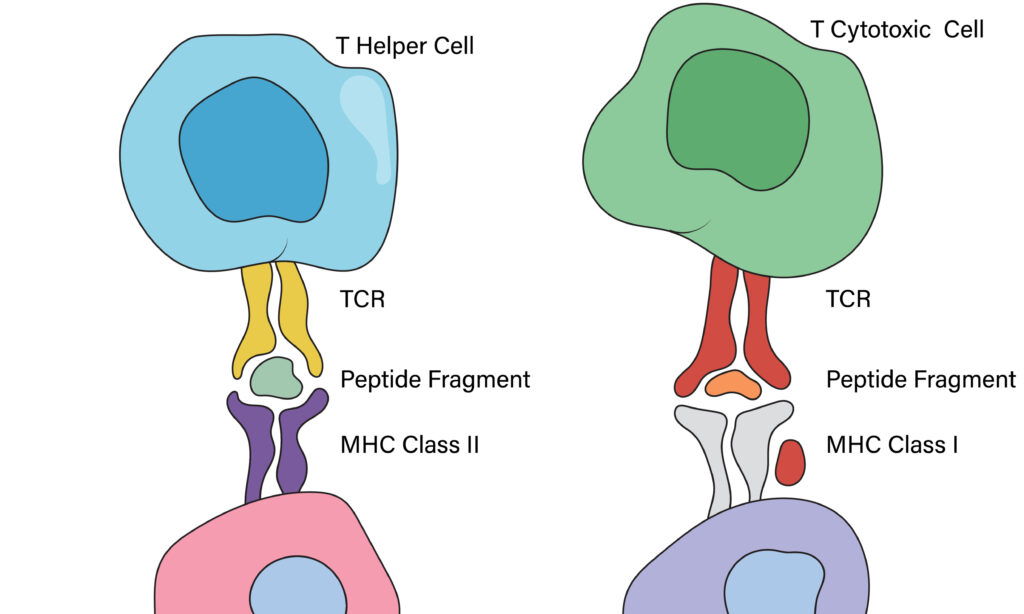
Proteasomes are machines inside our cells that help clean up damaged or faulty proteins and maintain protein homeostasis keeping the cell healthy. One highly specialized type of proteasome, called the immunoproteasome, is switched on during inflammation and disease processes. Immunoproteasomes work differently from others, breaking down proteins in a way that generates small antigenic peptides and helps the immune system recognise abnormal cells, such as those that are virally-infected or turning cancerous. This is important because immune cells, especially cytotoxic T-cells called CD8+ cells, know which cells to attack by detecting unusual protein fragments on the cell surface. Thus, if cancer cells don’t show these warning signs, they can escape detection.
Dr Driscoll and his team are working on a new approach to improve this process. They use special drug-like molecules to switch on immunoproteasomes. This helps cancer cells show a larger quantity, and more varied warning signals —also known as tumour antigens— on their surface. The goal is to make it easier for the immune system to recognize and destroy cancer cells that might otherwise go unnoticed.
Treatment of multiple myeloma is difficult because the cancer cells can hide from the immune system. One way they do this is by reducing the number of tumour antigens on their surface. Without these warning flags or signposts, treatments that rely on immune cells, such as immune checkpoint inhibitors and artificially manufactured T-cells (called CAR-T, or chimeric antigen receptor cells) are less effective.
The research team lead by Dr Driscoll found that pharmacologically turning on immunoproteasomes could help fix this problem. Acting like recycling units inside cells, immunoproteasomes break down proteins into smaller pieces, enabling these fragments to be used to alert the immune cells. By boosting this process, the researchers hoped to help myeloma cells display more surface warning signs for immune cells to see, and act on. Their results also showed that activating the immunoproteasome helped uncover new or hidden cancer signals (called neoantigens), which the immune system had previously missed.
Uncovering neoantigens made it easier for T-cells to recognize and destroy the cancer cells. These effects were seen in lab-grown myeloma cells and also in animal models created using real patient cancer cells. The treatment used killed cancer cells more effectively, and without causing harmful side effects, suggesting that this approach could offer a safer, more powerful way to treat multiple myeloma in the future.

Immunoproteasome Activators
To find new ways to help the immune system recognize and fight cancer, Dr Driscoll and his team tested over 9,000 small drug-like compounds. They found that a lead molecule, designed Compound A, enhances a key part of the immunoproteasomes called the β5i catalytic subunit, without harming healthy cells. Using advanced protein analysis, the team found that Compound A works by attaching to a specific part of the proteasome (called PSMA1) and helping it interact with two helper proteins (PA28α and PA28β). This interaction is essential, as confirmed by experiments in which blocking the activity of any of these three proteins stopped Compound A from working.
Further tests showed that treatment with Compound A greatly increased the number and variety of neoantigens presented on myeloma patient tumor cells, with some increased more than 100 times. The team also looked at another way to boost this system, by blocking a protein called histone deacetylase 6 or HDAC6, using drugs such as tubastatin A. These drugs activate the proteasome through a different route, but improving immune visibility in a similar way. These results support the idea that enhancing the immunoproteasome can make cancer cells easier to detect and destroy by the immune system — offering a promising new strategy in cancer immunotherapy.
Dr Driscoll and his team also explored inhibitors of HDAC6, an enzyme which removes a particular carbon molecule from proteins, effecting their function. In both tumour cell lines and mouse models of multiple myeloma, treatment with either Compound A or HDAC6 inhibitor drugs resulted in an increase in the number and variety of antigens on the surface of the cells. Tumour cells that were treated with Compound A before being implanted into mice grew into smaller tumours, especially when combined with T-cell therapy, and a similar benefit was seen with the HDAC6 inhibitors.
Interestingly, when immune cells were added to these treated cancer cells, cytotoxic activity increased further, regardless of whether the immune cells were from the same individual (autologous) or a different person (allogeneic). Importantly, this treatment did not result in an increase in the cancer cell defence mechanisms, which can arise during some treatments. Cancer cells often counterattack with the increased production of PD-L1, a molecule that can shut down immune cells. However, as a result of stable tumour cell behaviour in these experiments, the tumour cells become more visible to the immune system without making them harder to treat. These findings confirm that the immunoproteasome plays a vital role in helping the immune system recognize cancer, and could be key to boosting both natural and engineered T-cell therapies.

Therapeutic Implications for Cancer Immunotherapy and Combination Strategies
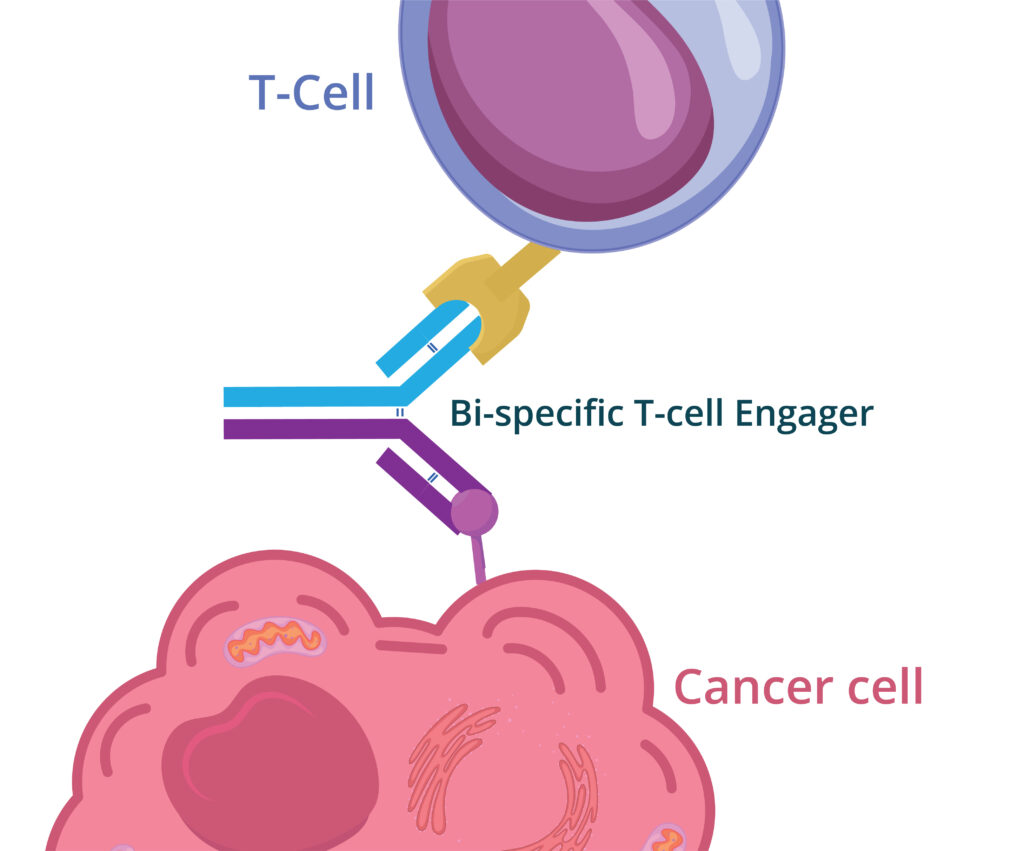
The implications of this work extend across the cancer immunotherapy landscape, with wide-reaching implications for how we treat hematologic cancers and solid tumours, using the immune system in adult and paediatric populations. Drugs that activate the immunoproteasome, like Compound A, help cancer cells become more visible to the immune system. This could improve the way some treatments work in patients who haven’t responded to standard therapies. One of the most exciting findings is that these drugs help uncover both shared cancer markers (found in many patients) and unique markers (specific to each individual). This makes them a promising tool for personalised cancer vaccines and advanced therapies, ones that train immune cells to target cancer more precisely — such as T-cell receptor therapies and bispecific T-cell engagers (BiTE), which bring immune cells directly to cancer cells.
This study also opens the door to powerful combination treatments. For example, pairing Compound A with checkpoint inhibitors (like anti-PD-L1 therapies) may help in cases where cancer cells hide by not showing enough warning signals. HDAC6 inhibitors, already being tested in clinical trials, may also boost immune responses in a different way — by changing how cancer genes are expressed and helping show more warning signals.
Overall, this approach supports the shift towards precision oncology — tailoring treatments to each patient’s unique cancer biology and genetic identity. Activating the immunoproteasome acts like turning up the volume on the immune system’s radar, helping it detect tumours that were previously hidden or resistant. It offers new hope for hard-to-treat cancers once thought to be invisible to the immune system. The results also reinforce the need for robust biomarker development, particularly around immunoproteasome subunit expression, as predictive tools to guide therapy selection for patients and monitor response.

Future Directions and Translational Research
Dr Driscoll and his team have made an important breakthrough in cancer research by showing that turning on the immunoproteasome can help the body better recognize and attack cancer. By using both new drugs (like Compound A) and existing medicines (such as HDAC6 inhibitors), they have established two mechanisms that boost how cancer cells show warning signals to the immune system. This improves the efficacy of current immune therapies, like T-cell treatments.
Their research opens the door to several exciting future directions. To bring Compound A into clinical use, scientists will first need to test how the drug behaves in the body and whether it’s safe. It may work best when combined with other immune therapies. They also plan to look for biological markers that can predict who will benefit most — for example, specific proteins or the number of neoantigens on tumour cells. This strategy could also be useful in treating other cancers, especially those that are harder for the immune system to detect. Beyond cancer, it may even apply to diseases like infections or neurodegenerative conditions, where immune recognition is key.
As technology improves — especially tools that help scientists map immune responses — treatments can become even more tailored to each patient. This research highlights the immunoproteasome not just as a cellular tool, but as a powerful target for therapy, one that could help reshape how we treat cancer and possibly other serious immune diseases.
SHARE
{kind=link}
DOWNLOAD E-BOOK
REFERENCE
https://doi.org/10.33548/SCIENTIA1215
MEET THE RESEARCHER
James J. Driscoll, MD, PhD
Seidman Cancer Centre, University Hospitals Cleveland Medical Center, Cleveland, OH, USA
James J. Driscoll is a physician-scientist at University Hospitals Cleveland Medical Center, Cleveland. He earned his MD and PhD from the University at Buffalo School of Medicine, undergoing internal medicine training affiliated with Boston University, and a hematology and oncology fellowship at the National Cancer Institute. Dr Driscoll is internationally recognized for his pioneering work on the proteasomes, and through his research has advanced understanding of how the immunoproteasome can be pharmacologically activated to enhance antigen presentation in cancer. He has identified and characterized novel small molecules that increase the catalytic activity of immunoproteasomes, leading to a dramatic increase in the presentation of MHC class I antigens and neoantigens on multiple myeloma (MM) cells. As a result, MM cells are much more susceptible to T-cell-mediated immunosurveillance and tumor lysis. These findings have significant implications for the development of immunotherapy and personalized cancer vaccines, and future treatment and prognosis. Using human and mouse model systems, they have identified commonly shared and patient-specific MHC class I neoantigens on MM tumor cells. The identification of shared neoantigens across patients provides a promising avenue to develop broadly applicable immunotherapies while the discovery of private antigens facilitates the development of personalized medicines. Neoantigens upregulated upon immunoproteasome activation can be exploited to expand the scope of TCR-engineered T-cells, T-cell engagers and cancer vaccines. Dr Driscoll’s translational work continues to shape therapeutic strategies across oncology and immune-related diseases, promising significant advances for patients and managing clinicians.
CONTACT
E: james.driscoll@uhhospitals.org
LI: https://www.linkedin.com/in/james-driscoll-b41484197
KEY COLLABORATORS
Dr James J. Ignatz-Hoover, Case Comprehensive Cancer Center, Case Western Reserve University
Dr Priyanka S. Rana, Case Comprehensive Cancer Center, Case Western Reserve University
Dr Ehsan Malek, Seidman Cancer Center, University Hospitals Cleveland Medical Center
Dr Yuriy Federov, Small Molecule Drug Discovery Core, Case Western Reserve University
Dr Drew J. Adams, Small Molecule Drug Discovery Core, Case Western Reserve University
Dr Timothy Chan, Lerner Research Institute, Cleveland Clinic
Dr Amber L. Mosley, Department of Biochemistry and Molecular Biology, Indiana University School of Medicine
FUNDING
NIH R01 Grant Number: 5R01AI139141
UH Seidman Cancer Center
Vinney Foundation
Case Comprehensive Cancer Center (Case CCC)
FURTHER READING
Driscoll, J.J. (2025) Abstract: Exploring molecular glues to activate proteasomes and develop personalized neoantigen-based therapeutics in multiple myeloma. Presentation at the International Myeloma Society, Toronto, Canada, 2025.
Rana, P.S., Ignatz-Hoover, J.J., Guo, C., et al. (2024) Immunoproteasome Activation Expands the MHC Class I Immunopeptidome, Unmasks Neoantigens, and Enhances T-cell Anti-Myeloma Activity. Molecular Cancer Therapeutics, 23(12), pp.1743–1760. https://doi.org/10.1158/1535-7163.MCT-23-0931.
Rana, P.S., Ignatz-Hoover, J.J., Kim, B.G., et al. (2024) HDAC6 Inhibition Releases HR23B to Activate Proteasomes, Expand the Tumor Immunopeptidome and Amplify T-cell Antimyeloma Activity. Cancer Research Communications, 4(6), pp.1517–1528. https://doi.org/10.1158/2767-9764.CRC-23-0528.
Rana, P.S., Ignatz-Hoover, J.J., Driscoll, J.J., et al. (2023) Targeting Proteasomes and the MHC Class I Antigen Presentation Machinery to Treat Cancer, Infections and Age-Related Diseases. Cancers, 15(23), p.5632. https://doi.org/10.3390/cancers15235632.

REPUBLISH OUR ARTICLES
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence (CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
SUBSCRIBE NOW
Follow Us
MORE ARTICLES YOU MAY LIKE
Professor Abraham P. Lee | Delivering Cancer Immunotherapy with Acoustic-Electric Precision, AESOP’s Fact not Fable
Chimeric Antigen Receptor (CAR) T-cell therapy offers life-saving potential, particularly against blood cancers, but severe side effects such as cytokine release syndrome (CRS) limit its safety. These toxicities are linked to uncontrolled CAR expression levels on the T-cell surface. Led by Professor Abraham P. Lee, researchers at the University of California, Irvine, have developed an advanced microfluidic system, called the Acoustic-Electric Shear Orbiting Poration (AESOP) platform, to precisely control the dose of genetic material delivered into primary T cells. This innovation promises safer, more homogeneous, and highly effective cellular immunotherapies.

Dr Ray Stewart | Barriers to Dental Care for People with Special Needs: A Crisis of Neglect and Inaction
For people with special healthcare needs, something as basic as visiting a dentist can be nearly impossible. A ground-breaking paper by researchers at the University of California, San Francisco (UCSF) exposes the scale of this crisis. By outlining potential paths forward, Dr Ray Stewart and Dr Ben Meisel offer hope for significant improvements in access to essential dental care.
Dr Liisa Laakso | Lighting the Way: Exploring Photobiomodulation to Ease MELAS
MELAS is a rare and serious genetic condition that affects how the body’s cells produce energy, leading to extreme fatigue, muscle weakness, and a range of other symptoms. With no cure currently available, treatment focuses only on managing complications.
A team of researchers led by Dr Liisa Laakso at the Mater Research Institute-University of Queensland, Australia, is exploring an innovative, non-drug therapy called photobiomodulation, which uses light to stimulate mitochondria to work more efficiently. This pioneering study will provide intial evidence on whether PBM can safely reduce fatigue and improve quality of life for people living with MELAS, paving the way for future clinical trials.

Professor John Paul Pezacki, PhD, FRSC (UK) | Engineering Proteins for the Prevention of Disease Progression
The way in which viruses invade and replicate within their hosts involves a multilayered system of protein-based interactions, and understanding the mechanisms at play is crucial when developing potential treatments. Utilising new techniques such as genetic code expansion, Professor John Paul Pezacki and his team of researchers at the University of Ottawa in Canada have designed a novel, highly specific artificial protein complex which can halt the progression of viral infections in human cells. They have identified and described a novel approach to wider preventative and restorative therapeutics in human disease.