
Professor Christopher Carlin | Using Technology to Transform Care for Patients with Respiratory Diseases
Managing chronic obstructive pulmonary disease is a global healthcare challenge. Professor Christopher Carlin, Consultant Physician and Clinical Lead for Respiratory Medicine at the National Health Service Greater Glasgow & Clyde, is tackling this issue head-on using digital tools, including artificial intelligence-based care and remote-managed technology. He is improving patients’ quality of life by developing more proactive approaches to preventative management to reduce hospital admissions and improve clinical outcomes.
The Challenge Posed by Chronic Obstructive Pulmonary Disease
According to the World Health Organization, chronic obstructive pulmonary disease (COPD) is the third leading cause of death worldwide. In 2019 alone, it caused 3.23 million deaths around the world and is projected to be the leading cause of death globally by 2030.
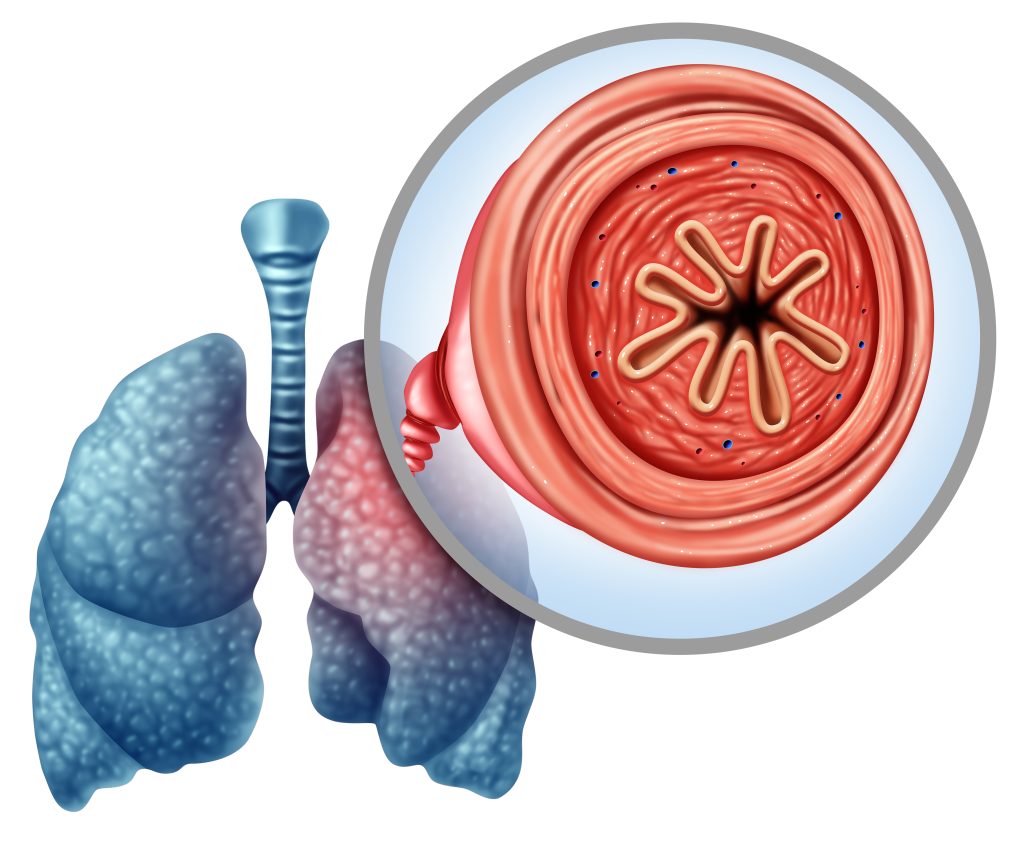
Linked to smoking and air pollution, COPD results in restricted airflow in the lungs. As the lungs become increasingly clogged with phlegm, patients experience a chronic cough, wheezing, difficulty breathing, and often feel tired. Unfortunately, there is no cure, although symptoms and risk of flare-ups can be improved by stopping smoking, reducing exposure to air pollution and personalised treatment. Available treatments include medicines, oxygen therapy, pulmonary rehabilitation, and vaccinations to prevent lung infections. As COPD progresses, patients can find it hard to carry on with their day-to-day activities, often experiencing breathlessness. The disease is also associated with a significant financial burden due to healthcare-related costs.
Professor Christopher Carlin, a respiratory medicine specialist based in Glasgow, is working to change the way that COPD is managed. He explains that COPD exacerbations – sudden flare-ups of the condition where breathing worsens (often caused by an infection) – are responsible for a large proportion of the disease burden, unwanted outcomes, and medical costs. Moving away from a reactive approach where patients experience worsening symptoms and then are treated (often in hospital) to a more proactive preventative method of care, in which the exacerbations are avoided in the first place, is needed.
Exploring the Potential Roles of Artificial Intelligence
The Topol Review commissioned by the National Health Service outlined recommendations to prepare the healthcare workforce to deliver a digital future using technologies to benefit patients. The report noted that advances in computing power and algorithm design have boosted the development of artificial intelligence (AI) based methods to analyse, interpret, and make predictions using healthcare data. There has also been a surge in interest in the potential clinical applications of AI, particularly in the field of respiratory medicine, with a significant amount of research on this published since 2016. Following on from this, Professor Carlin and his colleagues reviewed the current evidence available for the application of AI to COPD. They concluded that it holds great promise to improve healthcare outcomes, particularly regarding timely diagnosis and risk predictions in the mission to ensure proactive preventative care.
Professor Carlin explains that early and accurate diagnosis, along with personalised, predictive, preventative management, is required to address the challenges of COPD. He highlights that COPD has been identified as the ideal medical field to establish clinical, academic, and industrial partnerships in order to resolve variations in care using the development of AI solutions. He adds that such AI solutions could include interpretations of imaging and lung function tests to allow predictive applications. The understanding and recognition of COPD in its earliest stages (before symptoms appear) has progressed significantly such that an AI-based evaluation of chest computed tomography imaging could be used to identify COPD at this point, enabling far earlier interventions and, thus, slowing disease progression.
Helping Patients on Home Non-Invasive Ventilation
Non-invasive ventilation (NIV) uses a machine to help a patient to breathe. The patient has to wear a mask that covers their nose and mouth, which is connected to the NIV machine with a tube. The machine then maintains a set pressure to support a larger, more efficient breath. Professor Carlin states that COPD patients who have persistent hypercapnic respiratory failure have improved outcomes from long-term home NIV (these are patients with elevated levels of carbon dioxide in their blood because they cannot clear it properly due to their breathing difficulties). However, he highlights that providing home-NIV presents has its own set of challenges, as it needs careful monitoring and adjustments.
Professor Carlin and his team decided to investigate assistive technologies that could help these patients. They carried out a retrospective study to evaluate the outcomes of home NIV in hypercapnic COPD patients who had been set up at their centre using two-way remote monitored home-NIV in iVAPS-autoEPAP mode, a particular type of machine and mode which can allow automatic adjustments. The team analysed records of 46 patients with COPD who started remote-monitored home-NIV between February 2017 and January 2018, and compared data on the ‘time to readmission to hospital’ or ‘death at 12 months’ to a control group of 27 patients with the same condition who had not been referred for consideration for home-NIV, to allow a fair comparison for the study.
A Technology-Assisted Service Model
Professor Carlin found that the median time to hospital readmission or death was significantly prolonged in patients who started home-NIV, 160 days versus 66 days for the control group, plus the average time to hospital readmission was 221 days for the home-NIV patients versus 70 days. He adds that carbon dioxide levels were kept within a suitable range, and there were no increases in nurse home visits for the home-NIV patient group. In fact, reductions in healthcare usage were noted.
Professor Carlin concluded that remote monitoring using an ‘auto-titrating’ or ‘auto-NIV’ mode of home-NIV and two-way monitoring is not only feasible but has the potential to achieve the positive patient outcomes associated with NIV that have been achieved in previous studies. He goes on to explain that since the COVID-19 pandemic, remote management for respiratory care was mandated where possible, and this study was the first to offer an approach, demonstrate feasibility, and provide encouraging data supporting the use of a technology-assisted service model for home-NIV provision to patients with COPD.

Exploring a Digital Self-Management Support Service
Interventions that support COPD patients in self-managing their condition have been shown to reduce the length and frequency of hospital admissions, improve quality of life, reduce mortality, and demonstrate cost-effectiveness. However, Professor Carlin explains that clinical teams often lack the capacity to provide enough support for these interventions to be effective. Digital self-management services offer the opportunity to provide scalable access to resources that can supplement standard treatment as well as replace existing self-management programmes. While a wide range of digital COPD self-management interventions have been developed with positive results using internet- or application-based tools, methodological limitations such as small sample sizes and limited follow-up data mean insufficient evidence of significant, persisting benefit from these tools was available.
Professor Carlin and his colleagues conducted the RECEIVER trial to evaluate the Lenus COPD support service, a co-designed patient web application. They wanted to determine if patients with severe COPD would continue to use the tool throughout the study follow-up period and to explore the impact of this digital service on clinical outcomes with its adoption alongside routine care. The study began in September 2019 with 83 participants (referred to as the RECEIVER cohort) and included a suitable control group to compare clinical outcomes. The researchers determined utilisation by the completion of the daily COPD assessment test through the application, and they also collected and compared data on survival, hospitalisation, quality of life, symptom burden, and community-managed exacerbations for the two groups.
Exciting and Promising Results
Professor Carlin’s study found that the use of the application was high and sustained across the RECEIVER cohort, with an average follow-up of 78 weeks. A total of 64 out of the 83 patients in this group completed at least one COPD assessment test entry on ≥50% of possible follow-up weeks. Importantly, the median ‘time to death’ or ‘COPD or respiratory-related hospital admission’ was higher in the RECEIVER cohort compared to the control group – 335 days versus 155 days. A mean reduction was also found for ‘occupied bed days per year’ (a measure of bed occupancy used by hospitals; 8.12 days versus 3.38 days). Last but not least, the quality of life and symptom burden remained stable despite the progressive nature of COPD.
Professor Carlin and his colleagues concluded that their findings support the implementation of a scaled-up service provision to build proactive and preventative COPD care alongside continued evaluation of the digital service. Since the results were so promising, his team are now undertaking this scale-up implementation process.
Artificial Intelligence for Future Management
Professor Carlin says that the positive user experiences and useful datasets collated from the RECEIVER trial will support the development of future digital innovations, including the use of AI-derived insights. His next project, DYNAMIC-AI, will integrate digital innovations with remote management and predictive modelling for COPD care explored in the previous studies with AI-based insights. He will also determine the acceptability of such an intervention for COPD patients, as well as the technical feasibility and safety of using the Lenus COPD AI Insights application.
Although COPD remains a progressive disease, Professor Carlin’s continuing work to utilise technology offers genuine and significant potential to enhance the care for COPD patients and improve patient outcomes.
SHARE
{kind=link}
DOWNLOAD E-BOOK

REFERENCE
https://doi.org/10.33548/SCIENTIA980
MEET THE RESEARCHER

Professor Christopher Carlin
Department of Respiratory Medicine
Queen Elizabeth University Hospital
Glasgow
Scotland
Professor Christopher Carlin obtained his BSc in 1997, MB ChB in 2000, and PhD in 2009, all at the University of Glasgow in Scotland. In 2012, he became a Member of the Royal College of Physicians for Respiratory Medicine. He is a Consultant Physician for Sleep and Respiratory Medicine and the Clinical Lead for Respiratory Medicine at the National Health Service (NHS) Greater Glasgow & Clyde. He also holds the position of Honorary Professor in Respiratory Medicine at the University of Glasgow and is the NHS Research Scotland Senior Investigator for Respiratory Innovation. Professor Carlin runs a patient-focused respiratory medicine service and a research, innovation and training programme. On top of this, he has been a principal investigator in the West of Scotland Innovation Hub since its founding. He was the lead author for the 2020 Scottish Intercollegiate Guidelines Network guidance on continuous positive airway pressure in COVID-19 severe respiratory failure and has advised on the National Institute for Health and Care Excellence guidelines. Professor Carlin has led the utilisation of artificial intelligence technology, remote-managed monitoring, and digital services to care for patients with chronic obstructive pulmonary disease and severe respiratory failure.
CONTACT
E: christopher.carlin@ggc.scot.nhs.uk
W: https://woshealthinnovation.scot
T: @GSBSRC_QEUH
KEY COLLABORATORS
Professor David Lowe, University of Glasgow
Professor Sandosh Padmanabhan, University of Glasgow
FUNDING
Innovate UK
AI in Health and Care Award, NHS
Chief Scientist’s Office, NHS Scotland
FURTHER READING
A Taylor, A Cushing, M Dow, et al., Long-Term Usage and Improved Clinical Outcomes with Adoption of a COPD Digital Support Service: Key Findings from the RECEIVER Trial, International Journal of Chronic Obstructive Pulmonary Disease, 2023, 18, 1301–1318. DOI: https://doi.org/10.2147/COPD.S409116
G McDowell, M Sumowski, H Toellner, et al., Assistive technologies for home NIV in patients with COPD: feasibility and positive experience with remote-monitoring and volume-assured auto-EPAP NIV mode, BMJ Open Respiratory Research, 2021, 8(1), e000828. DOI: https://doi.org/10.1136/bmjresp-2020-000828
C Carlin, A Taylor, I Van Loon, et al., Role for artificial intelligence in respiratory diseases—chronic obstructive pulmonary disease, Journal of Hospital Management and Health Policy, 2021, 5, 27. DOI http://dx.doi.org/10.21037/jhmhp-20-119

REPUBLISH OUR ARTICLES
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence (CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
SUBSCRIBE NOW
Follow Us
MORE ARTICLES YOU MAY LIKE

Elevating Histology: Rethinking Clinical Laboratory Regulations for Modern Diagnostic Demands
Histology is the science dealing with the structure and analysis of cells and their formation into tissues and organs. The profession is responsible for the preparation of all pathological tissue samples removed and collected from the human body for the microscopic detection of tissue abnormalities for disease diagnosis and treatment. Despite advances in immunohistochemistry, molecular diagnostics, and digital pathology, the US Clinical Laboratory Improvements Amendments (CLIA) regulations from 1988 have not evolved to reflect histology’s scientific demands, including performing complex diagnostic tasks essential to patient care. Elizabeth Chlipala from Premier Laboratory (LLC), Longmont, Colorado and colleagues argue for a national certification requirement and regulatory oversight for histologists. Citing current problems including quality issues, workforce shortages, and the need for standardized practices, these experts argue that recognizing histologists under CLIA would elevate the profession, ensure competency, and improve patient outcomes, challenging the current position of the College of American Pathologists.
Dr Masumi Kamiyama | Using Natural Compounds from Soy to Protect Kidneys from Damage in Diabetes
Dr Masumi Kamiyama, Associate Professor at Jumonji University, Saitama, Japan, leads research into the early detection and prevention of diabetic nephropathy, which is kidney damage caused from long-term high blood sugar that makes it harder for the kidneys to filter waste, and can potentially lead to kidney failure. Dr Kamiyama and colleagues are exploring the role of a protein called angiotensinogen (AGT) as an early biomarker of kidney damage. The team studies the potential of plant-based antioxidants, called isoflavones, to slow or halt kidney damage from highly reactive molecules, such as oxygen free radicals. Ongoing research by Professor Han Lamers (University of Oslo) and Professor Bettina Reitz-Joosse (University of Groningen) reveals how Fascist Italy weaponized ancient Rome’s language to legitimise its power and connect Mussolini’s regime to Italy’s imperial past. Their projects involve collaboration with an international team of mostly junior researchers based in Norway, the Netherlands, Austria, and Italy.

Dr JoLee Sasakamoose – Dr Mamata Pandey | Empowering Indigenous Health: The Indigenous Wellness Research Collaborative in Saskatchewan
The Indigenous Wellness Research Collaborative is a transformative alliance dedicated to advancing health systems and service delivery for Indigenous communities across Saskatchewan. Founded a decade ago and co-led by Dr Mamata Pandey, a research scientist at the Saskatchewan Health Authority, and Dr JoLee Sasakamoose (M’Chigeeng First Nation), Canadian Institute of Health Research Chair in Indigenous Wellness and Health Equity at the University of Regina, their team’s work is rooted in a commitment to Indigenous leadership and community-defined wellness goals. Guided by the Cultural Responsiveness Framework, the Collaborative prioritises creating ethical spaces that serve as a middle ground for respect, reciprocity, and authentic partnerships. The team employs a strengths-based approach to health research, centering Indigenous methodologies that respect the interconnectedness of spiritual, mental, emotional, and physical well-being.

Professor Jaya Krishnan | Revolutionary Gene Therapy Helps Hearts Regenerate After Heart Attacks
Myocardial infarction, commonly termed as a heart attack, is a major cause of death and poor health worldwide. Regenerating heart tissue is an exciting and promising concept that can have significant benefits in myocardial infarctions and related diseases, but this has not yet been achieved in real-life clinical treatments. In a collaboration between Goethe University Frankfurt and Goethe University Hospital, Professor Jaya Krishnan and colleagues address this by controlling pathologic genes involved in the development of heart failure that develops after heart attacks. The researchers demonstrate a new way of treating heart disease by aiding in the division and regrowth of heart cells after a heart attack.