
Cancer Under Pressure: Managing Malignant Spinal Cord Compression
Malignant spinal cord compression is a common complication of advanced cancer, which can lead to major health problems if it is not discovered and treated urgently.
Professor Michael McKay is based at the North West Cancer Centre in Tasmania, and specialises in radiation oncology. He carries out vital research into how this potentially life-changing condition can be managed with radiotherapy and other approaches to identify the best evidence-based therapies for patients with this devastating diagnosis.
The Delicate Spinal Cord
Along with the brain, the spinal cord forms part of the central nervous system. A long, thin tube-like structure packed full of nervous tissue, it is housed in the spine and connects to the brain, enabling nervous communication throughout the body. Any damage to this delicate structure can result in signals to and from the brain being compromised, leading to life-changing problems such as loss of sensation and paralysis.
When cancer advances – becoming metastatic and spreading in the body – it can sometimes begin to grow in the spine. As the tumour becomes larger, it can eventually begin to compress the spinal cord, leading to potentially irreversible damage if it is not diagnosed and treated promptly. Professor Michael McKay provides radiation oncology services for the community of North West Tasmania, in Australia. He explains that malignant spinal cord compression (MSCC) is an oncological emergency which can be treated with various combinations of radiotherapy, steroids, and surgery. Correct diagnosis and management of MSCC, guided by the most up-to-date research, is vital to ensure the best outcomes for these patients.
Understanding the Pathology
Professor McKay highlights that while the frequency of MSCC is on the rise, this is most likely due to improvements in diagnosing the condition, and the fact that cancer therapies are also improving and patients are living longer. He says that MSCC occurs in 40% of patients whose cancer has spread to their bones. Usually, the main mechanism of damage is from the direct compression of the cord by the tumour, which most commonly grows in the epidural space, the small gap between the cord and spine. In the majority of cases, this occurs in the middle section of the backbone, the thoracic spine. He adds that the compression results in vasogenic oedema in the spinal cord (a build-up of fluid) and vascular injury impairing blood flow, and this will eventually cause tissue death. A quick resolution to the compression prevents this outcome.
Evidence-based Management
Professor McKay explains that surgery can be used in a small number of cases, but in general, radiotherapy and steroids are the main treatment options for MSCC. However, he stresses that current MSCC management needs to be re-evaluated for a number of reasons. Different radiotherapy prescriptions have only recently been examined in phase III clinical trials, and new approaches are emerging as a result of technological improvements in the delivery of radiotherapy. Additionally, modern systemic cancer therapies are also significantly boosting survival rates. The impact of these clinical trials and novel treatments needs to be carefully considered to guide the management of MSCC.
In light of recent clinical trials and new cancer treatments, Professor McKay and his colleague set out to provide a narrative review of the latest evidence in the diagnosis and management of MSCC. They searched numerous databases for all the papers about MSCC and the use of radiotherapy with or without surgery from 1970 through to 2023, and reviewed each one. Their report provided a detailed overview of the development of MSCC and its diagnosis, as well as a comprehensive summary of new approaches in its management.
Professor McKay explains that magnetic resonance imaging evaluating the whole spine is needed to give a full picture of the situation (in one-third of cases, multiple spine levels are affected) so informed clinical decisions can be made. Steroids reduce inflammation, in particular high doses of dexamethasone, with the short-term benefits almost always outweighing the potential side effects of these drugs. These can be given alone (rarely), alongside radiotherapy, or even with surgery followed by additional radiotherapy in certain circumstances. He adds that the indications for a patient’s suitability for surgery are narrow, and definitive data to guide the selection of surgery over radiotherapy alone remain limited.
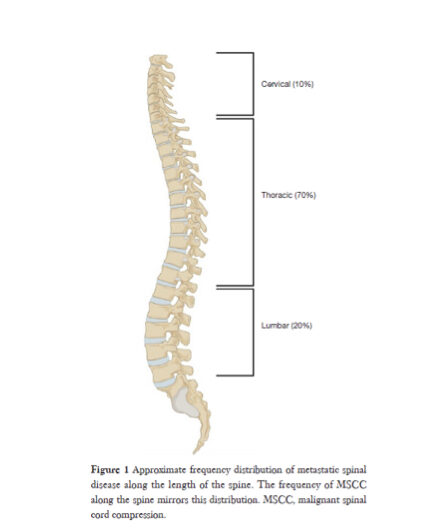
Approximate frequency distribution of metastatic spinal disease along the length of the spine. The frequency of MSCC along the spine mirrors this distribution.
Radiotherapy: A Cornerstone of Treatment
Radiotherapy uses high doses of radiation targeted at cancer cells in order to kill them and shrink the tumour. Alongside steroids, it is the cornerstone of MSCC treatment. Professor McKay highlights recent clinical trials exploring long versus short courses of radiotherapy, as well as stereotactic ablative radiotherapy (SABR), a highly focused and sophisticated type of radiotherapy which minimises damage to surrounding tissues. The report concluded that shorter radiotherapy courses could be considered for patients with a poor prognosis, and for patients with a more favourable prognosis, longer radiotherapy courses offer a more enduring control of the tumour.
Professor McKay notes that there is an emerging approach involving surgery combined with SABR, although it requires longer-term investigation. He adds that in addition to patient prognosis, other factors need to be taken into account when choosing the radiotherapy prescription. The degree of sensitivity of the tumour to radiotherapy, the amount of neurological impairment experienced by the patient, as well as the mechanical stability of the spine should all be considered. He concludes that treatment must be individualised based on thorough clinical assessment.
Future of MSCC Treatments
Estimated to occur in around 15% of cancer patients, particularly those with lung, breast and prostate cancers, MSCC significantly impacts health if not treated promptly. Professor McKay’s work in radiation oncology is helping to ensure a timely diagnosis and evidence-based treatment of MSCC, positively impacting the lives of many people living with cancer. He says the data from the studies on the emerging therapy of combining an operation called separation surgery with SABR suggest it provides very high rates of control for at least 1 year, and ablative doses of radiotherapy, which destroy tumour cells, appear to provide control of tumour types which are radioresistant.
Professor McKay highlights that using SABR by itself in the management of MSCC is, as yet, an understudied treatment. However, the limited data currently available suggest it has a role, and that the use of SABR needs further evaluation. He suggests that future studies could investigate the synergistic antitumour effects of combining SABR and systemic treatments, like immunotherapies, which use the patient’s own immune system to help fight the cancer, or targeted therapies for tumours which hold certain specific molecular markers.
SHARE
{kind=link}
DOWNLOAD E-BOOK

REFERENCE
https://doi.org/10.33548/SCIENTIA1218
MEET THE RESEARCHER

Professor Michael J McKay
Northern Cancer Service, North West Cancer Centre, Burnie, Tasmania, Australia
Professor Michael McKay initially trained in Radiation Oncology and then obtained his PhD from the University of Sydney and MD from the University of New South Wales. He next accepted an International Human Frontier Postdoctoral Fellowship in cancer genetics at the Department of Cell Biology and Genetics in Rotterdam. Here, he discovered several human genes which are involved in the body’s response to radiation, findings which formed the core of his translational research platform at the Peter MacCallum Cancer Centre in Melbourne, Australia. He was the Head of the DNA Repair Laboratory at this institution for 13 years, during which time he established and directed the Peter Mac Familial Cancer Centre. He later worked at the Australian National University and Royal Canberra Hospital, where he held the position of Professor of Radiation Oncology and Molecular Medicine. Additionally, he was a Clinical Professor at Sydney University and is currently an Honorary Professor at The University of Tasmania.
Professor McKay has been an Examiner and Chief Subject Examiner for the Royal Australian and New Zealand College of Radiologists for many years. He is currently a RANZCR Phase I examiner and Expert Reviewer. He has over thirty academic awards and honours. He is a member of the Northern Cancer Service Clinical Trials Oversight Committee and has served on working groups for the Trans Tasman Radiation Oncology Cancer Trials Research Group (TROG) and Clinical Trials Australia. He is an editorial board member for a number of journals and has given many national and international invited presentations. He has been the Chair/Convenor of many local and international meetings/symposia. Professor McKay has been a member of faculty for the ESTRO International courses on Clinical Radiobiology. He is Chair of the Cancer Council Tasmania Scientific and Research and is in full-time practice as a generalist Radiation Oncologist at the North West Cancer Centre in Tasmania. He has research interests in skin, urological, breast and central nervous system cancers.
CONTACT
E: michael.mckay@ths.tas.gov.au
KEY COLLABORATORS
Dr Zarique Akanda, Peter MacCallum Cancer Centre, Melbourne, Australia
FUNDING
Northern Cancer Service, Tasmania and Alfred Hospital, Department of Radiation Oncology, Melbourne, Australia
FURTHER READING
ZZ Akanda, MJ McKay, Narrative review—diagnosing and managing malignant epidural spinal cord compression: an evidence-based approach, Annals of Translational Medicine, 2023, 11(11), 386. DOI: https://dx.doi.org/10.21037/atm-22-3076
![]()
REPUBLISH OUR ARTICLES
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence (CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
SUBSCRIBE NOW
Follow Us
MORE ARTICLES YOU MAY LIKE

Jean Lycke | Addressing Unmet Medical Needs in Mucosal Disease: A Close-to-Market Innovation Approach
Recurrent Aphthous Stomatitis (RAS) is an oral condition characterized by one or several painful mucosal ulcers. RAS affects a large proportion of the population and has a point prevalence of approximately 2–3%, daily. The etiology remains unknown, and there is currently no curative treatment. Most patients experience recurring episodes over time, with each episode typically lasting up to a week. Here, we describe the development of a mucoadhesive patch which, when applied over a RAS ulcer, provides rapid pain relief. The patch is easy for patients to apply when symptoms begin and has the potential to be used as an over-the-counter product. The development of the Mucocort mucoadhesive patch is an example of a Close-to-Market innovation strategy that embraces simplicity within a complex healthcare system. By simplifying the product concept, the team has reduced the number of regulatory steps required before market approval. This MedTech/Pharma innovation model, known as the “4R” framework – Re-purposing, Re-formulation, Re-positioning, and Re-patenting – has guided the program from concept to commercialization. In addition to the biodegradable mucoadhesive patch developed for RAS ulcers, the team is extending the innovation concept to a mucoadhesive gel formulation for the prevention and treatment of chemotherapy-induced mucositis. This gel-based program is being commercialized separately through MucoShield.
The Translational Asian Agerelated Macular Degeneration Program Phase 2 (TAAP-2): Reimagining the Future of Vision Care
Age-related macular degeneration, often abbreviated as AMD, is one of the leading causes of vision loss among older adults worldwide. In Asia, where populations are ageing rapidly, its impact is particularly profound. For many, the disease quietly erodes central vision, making everyday activities such as reading, driving, and recognising faces increasingly difficult. Against this backdrop, the Translational Asian Age-related Macular Degeneration Programme, or TAAP for short, has emerged as a bold and ambitious effort to confront the disease headon. Now in its second phase, TAAP-2 represents a significant evolution in both scientific scope and clinical ambition.
Ms. Aikaterini Dritsoula | Looking Beyond Snoring: How Hidden Airway Problems Shape Children’s Sleep
For many parents, a child’s snoring may seem harmless, even endearing. Yet in some cases, it signals something more serious. Obstructive sleep apnoea is a condition in which a child’s breathing is repeatedly disrupted during sleep. These interruptions can affect growth, behaviour, and learning. Children with this condition may toss and turn at night, struggle to concentrate during the day, or show signs of hyperactivity and fatigue. Traditionally, enlarged tonsils and adenoids have been seen as the main culprits. Surgery to remove them has long been considered the standard treatment. However, research led by Consultant ENT Surgeon Ms. Aikaterini Dritsoula of The Leeds Teaching Hospitals NHS Trust invites us to look deeper. Her work suggests that the story is often more complex, especially in very young children.
Professor Neil Coffee – Professor Vincent Versace | Mapping Health Access: Using Address-Level Intelligence for Smarter Services
Accessing healthcare is a serious challenge for people living in rural and remote Australia. Large distances, sparse populations, and limited services can prevent residents from receiving care when they need it. Professors Neil Coffee and Vincent Versace at Deakin University’s Centre for Australian Research into Access (CARA) are leading research to model healthcare service access across the country, to provide new insights that can guide health planning and policy, as well as other services such as education. This work combines the curation of detailed address level residential dwellings and road network data to calculate access to service metrics (time and distance). These metrics are applied to the simulated residential dwelling population, to quantify the population with poor access to health services.