
Professor Antonio Bertoletti | The Perfect Storm: How Breakthrough virus Infections Create Superior Nasal Immunity
The nasal cavity serves as the primary entry point for SARS-CoV-2 and other respiratoy viruses, making it a critical frontline for immune defence. Professor Antonio Bertoletti from Duke-NUS Medical School in Singapore has been investigating how our immune systems respond to SARS-CoV-2 infection and vaccination. His groundbreaking research reveals that individuals who experience breakthrough SARS-CoV-2 infections after vaccination develop a uniquely robust ‘hybrid immunity’ in their nasal passages. This work provides crucial insights into developing more effective vaccines and enhances our understanding of why some people may be better protected against future infections than others.
The Gateway to Infection
When SARS-CoV-2 enters our body, it first encounters the cells lining our nasal passages. These nasal epithelial cells are particularly vulnerable to infection due to the abundance of ACE-2 receptors on their surface – the exact entry point the virus uses to infiltrate cells. This makes the nasal cavity not only the primary site of infection but also the main launching pad from which the virus can spread.
The initial phases of viral replication within these nasal cells are critical. If the immune system can mount a rapid and effective response at this stage, it may contain the infection before it can spread further. Based at Duke-NUS Medical School in Singapore, Professor Antonio Bertoletti has focused on understanding what makes an effective immune response in this crucial nasal environment, revealing that the location of immune cells matters tremendously.
Understanding the Immune Battlefront
Our immune system employs different types of cells to combat invading pathogens. Among these defenders are specialised white blood cells called T cells, which play a vital role in fighting viral infections. Unlike antibodies, which primarily target free-floating viruses, T cells can identify and eliminate cells that have already been infected.
T cells come in two main varieties: CD8+ T cells (often called ‘killer T cells’) can directly destroy infected cells, while CD4+ T cells (known as ‘helper T cells’) coordinate the broader immune response. Both types are crucial for effective antiviral immunity. T cells can develop memory – after encountering a particular virus, they can persist in the body for months or even years, ready to mount a rapid response if the same pathogen is encountered again. Intriguingly, T cells can also become ‘resident’ in specific tissues, serving as sentinels at common infection entry points like the respiratory tract.
The Vaccine and Infection Conundrum
Current COVID-19 vaccines are administered through intramuscular injection in the arm, primarily stimulating systemic immunity – generating antibodies and T cells that circulate throughout the bloodstream. While highly effective at preventing severe disease, this systemic approach has limitations when it comes to preventing initial infection at the nasal entry point. Natural infection, on the other hand, begins in the respiratory tract, triggering local immune responses directly at the site of viral entry. This local response includes the development of tissue-resident memory T cells that remain stationed in the nasal passages.
Professor Bertoletti thought that the ideal scenario might be a combination of both approaches – the broad systemic immunity provided by vaccination, complemented by the localised mucosal immunity triggered by natural infection. This combination, termed ‘hybrid immunity’, could potentially offer superior protection.
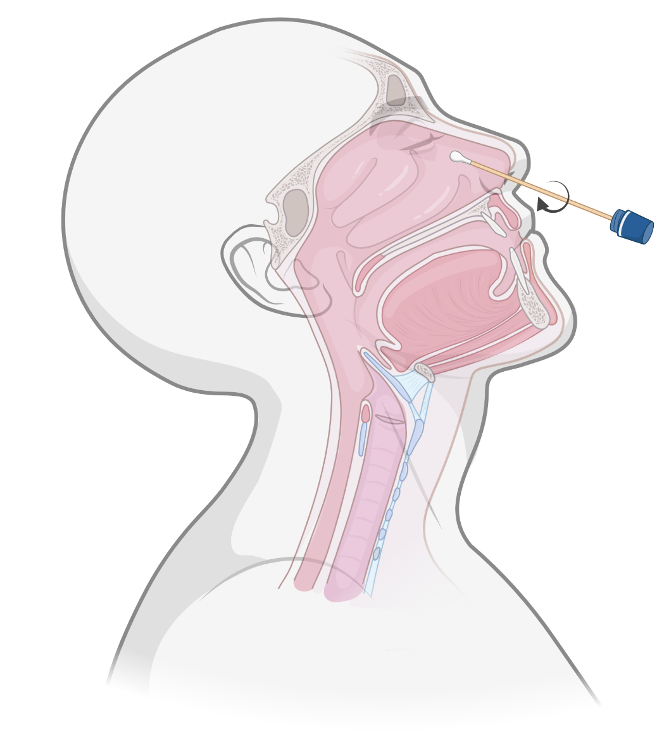
Rapid collection of T cells from
the human nasal cavity.
Discovering the Power of Hybrid Immunity
To test this hypothesis, Professor Bertoletti and his colleagues conducted a study investigating the nasal immune responses in different groups: those who had been vaccinated but never infected (naive vaccinees) and those who had experienced breakthrough infections after vaccination (convalescent vaccinees).
Their findings were remarkable. The naive vaccinees showed virtually no detectable SARS-CoV-2-specific T cells in their nasal passages despite having robust T cell responses in their blood. In stark contrast, almost all of the convalescent vaccinees exhibited strong SARS-CoV-2-specific T cell responses in their nasal mucosa. This broader recognition profile potentially offers more comprehensive protection, especially against viral variants with mutations in the spike protein.
Beyond the Spike: A Broader Immune Recognition
One of the most significant findings concerns the breadth of viral recognition by T cells after breakthrough infection. Current COVID-19 vaccines primarily target the spike protein of SARS-CoV-2. Natural infection, however, exposes the immune system to the entire viral repertoire – including structural proteins like nucleocapsid and membrane, as well as non-structural proteins.
Professor Bertoletti’s team found that the nasal-resident T cells in convalescent vaccinees recognised not only spike proteins but also these other viral components. Remarkably, in many individuals, the dominant T cell responses were actually directed against non-spike proteins – specifically nucleocapsid protein or NSP12. This broader recognition profile offers potential advantages. Since non-spike proteins tend to be more conserved across different viral variants, T cells targeting these components might maintain effectiveness even against heavily mutated variants that could evade spike-focused immunity.
The Importance of Natural Infection in Establishing Nasal Immunity
Perhaps the most striking finding was the apparent necessity of natural infection for establishing robust T cell immunity in the nasal mucosa. Despite receiving multiple vaccine doses, individuals who had never experienced SARS-CoV-2 infection showed essentially no detectable virus-specific T cells in their nasal passages. This finding highlights a fundamental limitation of current vaccination approaches: while highly effective at generating systemic immunity and preventing severe disease, parenteral (injected) vaccines appear poorly suited to establishing local immunity at respiratory entry points.
Professor Bertoletti’s team demonstrated this conclusively by tracking individuals longitudinally, before and after breakthrough infection. In these individuals, breakthrough infection led to the rapid appearance of SARS-CoV-2-specific T cells in the nasal mucosa, where none had been detectable beforehand. These findings have profound implications for vaccination strategies. They suggest that while current vaccines provide excellent protection against severe disease, they may be fundamentally limited in their ability to prevent initial infection and transmission.
The Persistence of Nasal Immunity
SARS-CoV-2-specific nasal T cells remained detectable for at least 3 months after breakthrough infection. However, when the researchers extended their tracking further, they found that most SARS-CoV-2-specific nasal T cell responses eventually waned to undetectable levels. This decline may be linked to the absence of key transcription factors, such as TCF-1 and EOMES, which are required for the long-term renewal of T cells. Yet one striking exception remained: a nasal T cell response against NSP12 that persisted for more than 4 years. Importantly, this response targeted an epitope fully conserved across all betacoronaviruses. This may mean that repeated exposures to respiratory viruses may help sustain certain populations of nasal-resident T cells, even in the face of intrinsic barriers to their long-term maintenance.
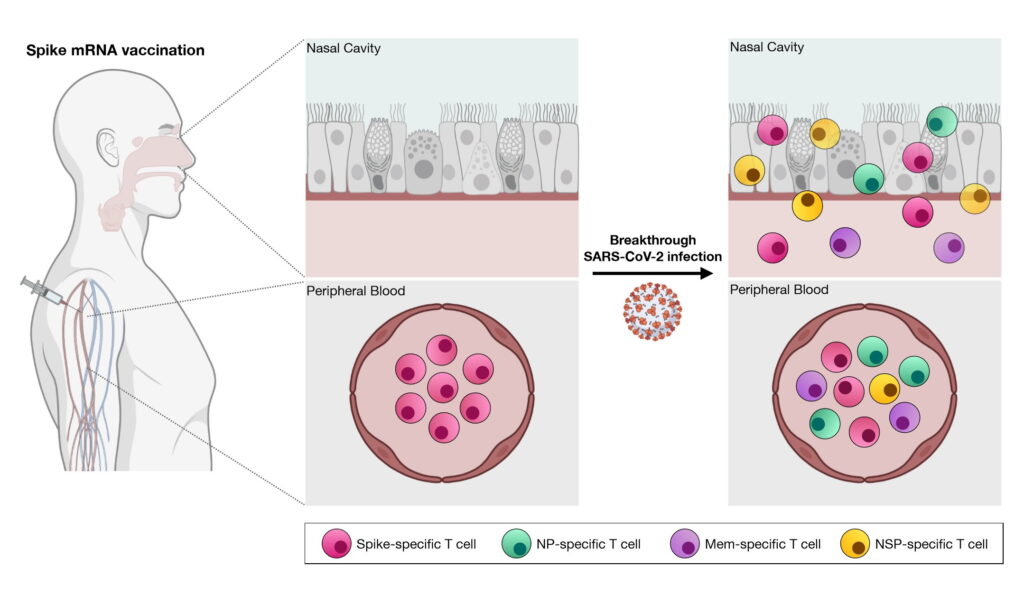
Viral challenge (breakthrough infection) is necessary to induce SARS-CoV-2-specific T cells in the nasal cavity of COVID-19 vaccinated individuals.
Implications for Future Vaccination Strategies
These discoveries have important implications for the future of COVID-19 vaccination strategies. While current vaccines have been remarkably successful at preventing severe disease and death, their limited ability to induce mucosal immunity represents a significant gap in protection.
The clear demonstration that natural infection induces robust T cell immunity in the nasal mucosa points toward potential improvements in vaccine design. It suggests that vaccines delivered directly to the respiratory mucosa – through intranasal administration – might be more effective at preventing initial infection and transmission than current injectable vaccines. However, the T cell response in the nasal mucosa is complex, and this complexity may pose challenges to developing an effective and long-lasting intranasal vaccine.
Several intranasal COVID-19 vaccines are currently in development, with some already approved for use in certain countries. Another approach might be prime-boost strategies that combine parenteral and mucosal vaccination.
Lessons for Future Pandemics?
This research has revealed the critical importance of nasal-resident T cells in protecting against SARS-CoV-2 infection and has demonstrated that these cells are effectively induced by breakthrough infection but not by parenteral vaccination alone. This understanding of ‘hybrid immunity’ helps explain why individuals who have experienced both vaccination and infection often show superior protection against subsequent exposures.
The work highlights a fundamental limitation of current COVID-19 vaccines. While highly effective at preventing severe disease through systemic immunity, these vaccines do not establish the local immune responses at the nasal entry point that might prevent initial infection and transmission. This insight points toward potential improvements in vaccination strategies, particularly the development of mucosal vaccines that specifically target immunity at respiratory surfaces.
As we continue to face the challenges of SARS-CoV-2 and other respiratory viruses, Professor Bertoletti’s research provides a valuable roadmap for developing more comprehensive immune protection. By understanding the complex interplay between different types of immunity and their anatomical distribution, we may be able to design next-generation vaccines that not only prevent severe disease but also more effectively block infection and transmission at its source.

Novel intranasal vaccine can be administered directly into the nasal cavity.
SHARE
{kind=link}
DOWNLOAD E-BOOK

REFERENCE
https://doi.org/10.33548/SCIENTIA1237
MEET THE RESEARCHER
Professor Antonio Bertoletti
Programme in Emerging Infectious Diseases, Duke-NUS Medical School, Singapore

Professor Antonio Bertoletti obtained his medical degree from the University of Parma in Italy. He specialised in infectious diseases, carrying out research into the hepatitis B virus at The Scripps Research Institute in La Jolla, and later returned to Parma to work as Clinical Scientist in the Department of Infectious Diseases. In 1995, he joined the MRC Unit in the Gambia as Senior Immunologist and then undertook the role of Senior Lecturer at the Institute of Hepatology at University College London. In 2006, he accepted the position of Director of Infection and Immunity Programme at the Singapore Institute for Clinical Sciences (A*STAR), and in 2013 became full Professor at the Emerging Viral Disease Programme at Duke-NUS Medical School. In 2015 Professor Bertoletti founded the Lion TCR Pte, a biotech company developing immune-based treatments for virus-related cancers and chronic viral infections. He has received numerous awards, including three consecutive terms of the Singapore Translational Research Awards and the European Association Study of Liver (EASL) 2023 Recogntion Award. An expert in viral hepatitis, he has a specific interest in the immunopathogenesis of HBV infection, and his research focuses on the development of new immunological-based therapies for chronic HBV infections and hepatocellular carcinoma.
CONTACT
E: antonio@duke-nus.edu.sg
KEY COLLABORATORS
We thank the Dr Jenny Low and all the staff of Department of Infectious Diseases, Singapore General Hospital for their tireless work in coordinating the collection of nasal samples. We would also like to extend our heartfelt thanks to all the donors for agreeing to participate in our research.
FUNDING
We thank the Singapore Ministry of Health (MOH) under PREPARE Research Fund (PREPARE-CS1-2022-007) and the National Medical Research Council (NMRC) Singapore Translational Research Investigator Award (STaR) MOH-001633 (STaR24jan-0004) which provided the funds for the research highlighted in this article.
FURTHER READING
Lim JME, Ottolini S, Hang SK, et al. Dynamics of virus-specific CD8+ T cells in the human nasal cavity. Mucosal Immunol. Published online July 22, 2025. doi:10.1016/j.mucimm.2025.07.007
Lim JME, Tan AT, Le Bert N, Hang SK, Low JGH, Bertoletti A. SARS-CoV-2 breakthrough infection in vaccinees induces virus-specific nasal-resident CD8+ and CD4+ T cells of broad specificity. J Exp Med. 2022;219(10):e20220780. doi:10.1084/jem.20220780
![]()
REPUBLISH OUR ARTICLES
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence (CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
SUBSCRIBE NOW
Follow Us
MORE ARTICLES YOU MAY LIKE

Assoc Prof. Nicholas Brown | Rethinking Prostate Care: A New Frontier in Treating Benign Prostatic Hyperplasia
For millions of men, ageing brings with it a set of frustrating and often disruptive urinary symptoms. These symptoms, caused by benign prostatic hyperplasia, or BPH, can affect sleep, confidence, and overall quality of life. Traditionally, treatment follows a familiar path. Patients begin with medications, often for years, and may eventually progress to surgery if symptoms worsen. Yet this pathway is not without its drawbacks. Medications can cause side effects, while surgery carries risks and recovery time. In recent years, a minimally invasive interventional radiology procedure called prostate artery embolisation, or PAE, has begun to challenge this traditional model. At the forefront of this shift is a collaborative research group, led by Dr. Nicholas Brown of the University of Queensland, whose series of P-EASY studies has explored whether PAE could transform how BPH is treated, particularly at earlier stages.

Jean Lycke | Addressing Unmet Medical Needs in Mucosal Disease: A Close-to-Market Innovation Approach
Recurrent Aphthous Stomatitis (RAS) is an oral condition characterized by one or several painful mucosal ulcers. RAS affects a large proportion of the population and has a point prevalence of approximately 2–3%, daily. The etiology remains unknown, and there is currently no curative treatment. Most patients experience recurring episodes over time, with each episode typically lasting up to a week. Here, we describe the development of a mucoadhesive patch which, when applied over a RAS ulcer, provides rapid pain relief. The patch is easy for patients to apply when symptoms begin and has the potential to be used as an over-the-counter product. The development of the Mucocort mucoadhesive patch is an example of a Close-to-Market innovation strategy that embraces simplicity within a complex healthcare system. By simplifying the product concept, the team has reduced the number of regulatory steps required before market approval. This MedTech/Pharma innovation model, known as the “4R” framework – Re-purposing, Re-formulation, Re-positioning, and Re-patenting – has guided the program from concept to commercialization. In addition to the biodegradable mucoadhesive patch developed for RAS ulcers, the team is extending the innovation concept to a mucoadhesive gel formulation for the prevention and treatment of chemotherapy-induced mucositis. This gel-based program is being commercialized separately through MucoShield.
The Translational Asian Agerelated Macular Degeneration Program Phase 2 (TAAP-2): Reimagining the Future of Vision Care
Age-related macular degeneration, often abbreviated as AMD, is one of the leading causes of vision loss among older adults worldwide. In Asia, where populations are ageing rapidly, its impact is particularly profound. For many, the disease quietly erodes central vision, making everyday activities such as reading, driving, and recognising faces increasingly difficult. Against this backdrop, the Translational Asian Age-related Macular Degeneration Programme, or TAAP for short, has emerged as a bold and ambitious effort to confront the disease headon. Now in its second phase, TAAP-2 represents a significant evolution in both scientific scope and clinical ambition.
Ms. Aikaterini Dritsoula | Looking Beyond Snoring: How Hidden Airway Problems Shape Children’s Sleep
For many parents, a child’s snoring may seem harmless, even endearing. Yet in some cases, it signals something more serious. Obstructive sleep apnoea is a condition in which a child’s breathing is repeatedly disrupted during sleep. These interruptions can affect growth, behaviour, and learning. Children with this condition may toss and turn at night, struggle to concentrate during the day, or show signs of hyperactivity and fatigue. Traditionally, enlarged tonsils and adenoids have been seen as the main culprits. Surgery to remove them has long been considered the standard treatment. However, research led by Consultant ENT Surgeon Ms. Aikaterini Dritsoula of The Leeds Teaching Hospitals NHS Trust invites us to look deeper. Her work suggests that the story is often more complex, especially in very young children.