
AI-Based Video Monitoring of Movement Disorders: Improving Care for Patients with Parkinson’s Disease
As our global population ages, movement disorders like Parkinson’s disease present growing challenges for healthcare systems. Traditional assessment methods rely on subjective clinical ratings during brief clinic visits and often fail to capture the full picture of a patient’s condition. Professor Martin McKeown and his colleagues are pioneering innovative artificial intelligence approaches which use ordinary video recordings to objectively monitor movement disorders. These cutting-edge technologies promise to transform care for millions of patients by enabling remote, continuous assessment of symptoms, while reducing healthcare costs and improving quality of life.
The Growing Challenge of Movement Disorders in an Ageing Population
The worldwide increase in elderly populations has created an unprecedented challenge for healthcare systems. As people age, they become increasingly vulnerable to chronic neurological conditions that can severely impact their mobility and quality of life. Particularly concerning are chronic movement disorders such as Parkinson’s disease (PD) and essential tremor (ET), which impose significant social and economic burdens globally.
PD is characterised by resting tremor, bradykinesia (slowness of movement), rigidity, and postural instability, and it affects up to 1% of people over 65 years of age. ET is the most common movement disorder, characterised by bilateral action and postural tremors that primarily affect the upper limbs.
Despite their debilitating effects, the clinical assessment of these conditions remains surprisingly archaic. While most medical disorders are monitored through objective laboratory or imaging tests, determining the progression of PD and ET relies largely on medical history and neurological examination.
The Limitations of Traditional Assessment Methods
The traditional assessment of movement disorders faces several critical challenges that limit effective patient care. Professor McKeown, Dr Maryam Mirian, and their colleagues at the University of British Columbia have identified key issues with the current clinical approach. The gold standard for measuring severity is based on clinical rating scales – like the Movement Disorder Society’s Unified Parkinson’s Disease Rating Scale (MDS-UPDRS) for PD, or the Tremor Research Group Essential Tremor Rating Scale (TETRAS) for ET. These scales require clinicians to assign scores ranging from 0 (none) to 4 (severe) for various symptoms based on personal observation and assessment, making them inherently subjective and potentially inconsistent between evaluators.
Additionally, PD patients typically experience motor fluctuations throughout the day in response to their medication schedules. Professor McKeown points out that a single visit to the clinic captures merely a momentary snapshot of the patient’s condition, which may not accurately represent their overall disease severity. This can lead to treatment decisions based on incomplete information. Even among experienced neurologists, the premortem identification of PD stage hovers around 80%. The definitive assessment requires postmortem identification of Lewy bodies in the substantia nigra, which is not practical for guiding treatment during a patient’s life.
Unlocking the Advantages of AI-Powered Video Monitoring
To overcome these limitations, the team has been exploring how artificial intelligence can revolutionise the assessment of movement disorders. The field has seen rapid advancement, particularly with the development of wearable sensor technologies that collect real-time patient data. However, wearable technology has its limitations, particularly regarding patient compliance. Not all patients consistently wear the devices, leading to gaps in data collection. This has prompted researchers to explore alternative, less intrusive methods of assessment.
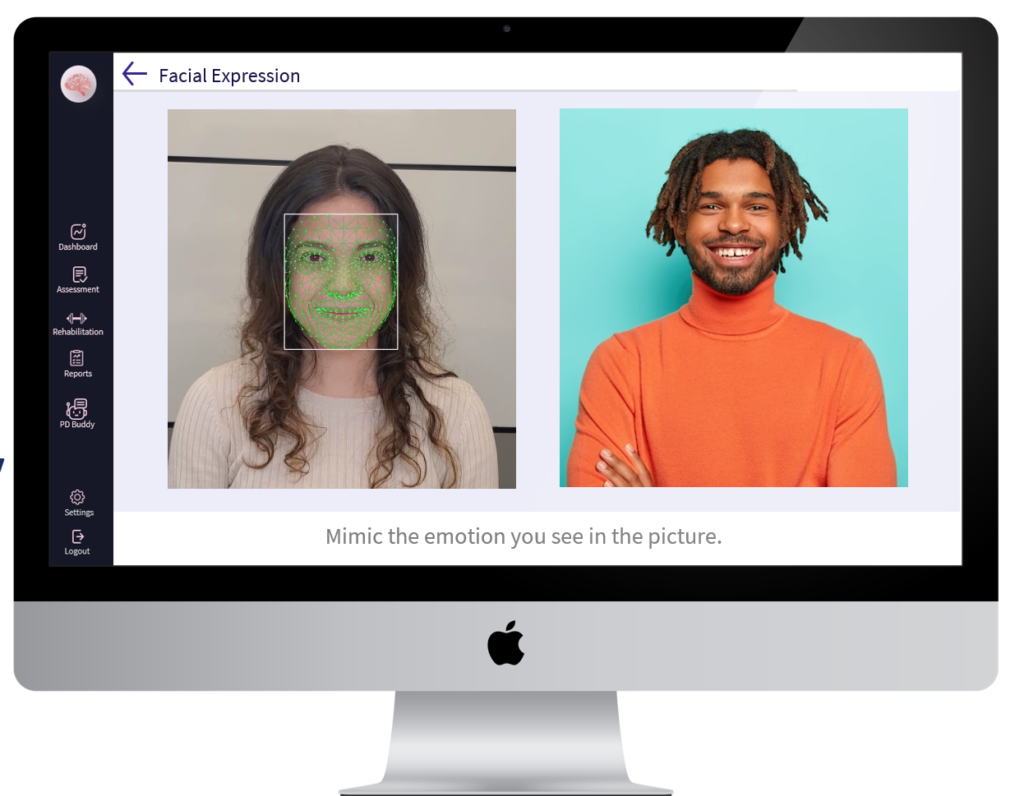
Video-based monitoring using computer vision technologies has emerged as a promising approach. By simply recording patients performing specific tasks or during everyday activities, these systems can analyse movement patterns without requiring patients to wear any devices. Professor McKeown emphasises that this non-intrusive nature is particularly beneficial for elderly patients who may struggle with the technical aspects of wearable devices.
The team’s research highlights several significant advantages of AI-powered video monitoring for movement disorders, particularly for elderly patients. Remote monitoring allows patients to collect real-time data in their own environments without frequent hospital visits. This is especially valuable for elderly patients who have mobility issues or live in rural areas with limited access to specialists. The COVID-19 pandemic further underscored the importance of such remote assessment capabilities.
The AI models analyse data objectively, eliminating the possibility of inter-rater or intra-rater variability that affects traditional clinical assessments. This results in more consistent evaluations over time, allowing for more accurate tracking of disease progression. Clinical trials for new treatments can benefit enormously from these technologies. Professor McKeown explains that the enhanced objectivity and statistical rigour of AI-assisted monitoring systems facilitate more accurate assessments of treatment efficacy, potentially accelerating the development of new therapies. Doctors can track fluctuating symptoms throughout the day since data can be collected continuously rather than only during clinic visits. This provides a more comprehensive picture of the patient’s condition, enabling more personalised treatment plans.
The system reduces the burden on medical staff by automating data collection and analysis, allowing healthcare providers to focus more on direct patient care and complex medical tasks. Meanwhile, patients can undergo monitoring from the comfort of their homes, reducing travel-related stress and expenses. For elderly patients, in particular, video-based monitoring offers advantages over sensor-based approaches. This does not require wearing devices, allowing for purely passive, non-intrusive monitoring of daily activities.
Video-Based Assessment of Movement Disorders
The research team are at the forefront of developing and evaluating video-based methods for assessing movement disorders. They examined ten recordings that used markerless consumer-level videos with AI models for PD assessments. These experiments typically follow a three-step process: pose estimation, kinetic feature extraction, and classification.
In the first step, pose estimation, the AI identifies key body joints and landmarks from the video. This creates a skeletal representation of the person’s posture and movements. Many studies use open-source libraries such as OpenPose or MediaPipe to accomplish this task. The second step involves extracting meaningful kinetic features from the estimated poses. These features represent clinical characteristics such as amplitude, velocity, and decremental responses during repeated movements, which are key indicators of movement disorders. Finally, the classification step uses machine learning algorithms to analyse these features and predict the severity of the condition or distinguish between healthy individuals and those with movement disorders.
The team notes that this approach differs from the ‘black-box’ AI models commonly used in some medical imaging applications. Instead of directly predicting a diagnosis from raw images, these systems extract specific movement features that align with what clinicians look for during assessments. This makes the results more interpretable and clinically relevant. For example, when assessing Parkinsonian gait, the system analyses features such as stride amplitude, stride speed, height of foot lift, heel strike during walking, turning, and arm swing. For tremor, it examines amplitude, frequency, and duration. For bradykinesia, it looks at amplitude, velocity, and decrement during repeated movements and hesitations.
Innovative Research Approaches
Indeed, a particularly innovative aspect of the team’s research is the development of weakly supervised learning methods for analysing PD videos, such as gait. Traditional fully-supervised learning approaches require many hand-labelled examples, which can be time-consuming and expensive to produce, especially in medical applications where expert annotation is needed.
The team has developed a novel approach that does not require extensive clinician-annotated training data. Instead, their method uses domain-specific knowledge obtained from neurologists to define labelling functions that identify key movement characteristics. Their system uses several labelling functions to classify patients’ gait based on features such as arm swing symmetry, step length, foot clearance, hip and knee flexion, trunk rotation, step width, and cadence. These labelling functions generate ‘noisy’ labels that are then refined using a generative model to learn the accuracy of each function. The researchers demonstrated that this weakly-supervised approach could achieve an accuracy of 89% in labelling PD from gait videos without requiring any clinical labels for training. This marks a significant improvement over previous methods, which typically required extensive labelled data.
Another important contribution involves the analysis of hand movements in PD patients. Professor McKeown developed PA-Tran, a novel deep learning framework for 3D hand pose estimation from a single RGB image using partial annotation. The system consists of two interconnected branches: a classification branch that predicts whether each keypoint is visible, and a regression branch that estimates the 3D coordinates of the keypoints. The team found that PA-Tran outperformed existing methods, achieving more accurate hand pose estimation even with partially visible hands.
Towards Home-Based Monitoring
Looking to the future, the researchers envision a progression towards discreet, home-based evaluations of movement disorders during routine daily activities. Rather than requiring patients to perform specific tasks, future systems will automatically modularise movement patterns and assess impairment in each movement as patients go about their everyday lives.
However, several steps are needed to realise this vision. First, data must be acquired in unrefined, free-living conditions capturing complex movements of daily activities. Second, these complex movements need to be automatically classified into specific modules (such as walking, eating, and dressing), and the degree of impairment for each action should be automatically measured. Third, this assessment should strongly correlate with how individuals actually feel about their impairments. Most importantly, all these advances must occur within secure ethical and regulatory boundaries, with careful attention to data security, privacy protection, and adherence to evolving standards.
Challenges and Potential Pitfalls
Despite the promising potential of video-based monitoring, Professor McKeown and his colleagues have identified several challenges that must be addressed for successful implementation. Video quality can significantly affect the performance of AI models. Factors such as resolution, lighting conditions, camera angles, motion blur, and network glitches can all impact the accuracy of the analysis. The team demonstrated this in a study where they simultaneously recorded finger-tapping movements under various resolution and network environments using Zoom. They found that remote video recordings varied considerably in quality, leading to significant errors in automated movement analysis. Another issue is that the model’s performance is highly dependent on the quality of the training data. Since there is high inter-rater variability from clinical assessments, it can be difficult to determine the “ground truth” labels to accurately train the AI models. The team’s approach to mitigating this is the use of weak supervision.
Privacy protection is a primary ethical concern with video-based monitoring. Video recordings capture identifiable information, including face, voice, and surroundings. A possible solution could be implementing automated camera-end preprocessing to extract only key body information while discarding other potentially identifying details. Interestingly, the team found that elderly PD patients were surprisingly positive about continuous home-based video recording, provided their privacy was secured, and they could turn off the camera at their discretion. This suggests that patients recognise the potential benefits of this technology despite privacy concerns.
Transforming Care for Movement Disorder Patients
The innovative work of Professor McKeown, Dr Mirian, and their colleagues represents a significant step forward in how we assess and monitor movement disorders. It highlights the technical possibilities of AI-based video monitoring and the importance of developing these tools with a deep understanding of clinical needs and patient perspectives. The path forward involves continued refining of these technologies, careful attention to ethical considerations, and close collaboration between technical experts and healthcare providers. As these systems mature and become more integrated into clinical practice, they have the potential to significantly improve the quality of life for millions of people living with movement disorders worldwide.
SHARE
{kind=link}
DOWNLOAD E-BOOK

REFERENCE
https://doi.org/10.33548/SCIENTIA1263
MEET THE RESEARCHER

Dr. Martin J. McKeown
Division of Neurology, University of British Columbia, Vancouver, Canada
Professor McKeown is the John L. Nichol Chair in Parkinson’s Research and Professor and Head of the Division of Neurology at the University of British Columbia. With a multidisciplinary background spanning Engineering Physics, Medicine, Neurology, and Computational Neuroscience, he received training at McMaster University, the University of Toronto, the University of Western Ontario, and the Salk Institute for Biological Studies. Professor McKeown’s research integrates medical and engineering principles to advance the understanding of Parkinson’s disease, develop innovative non-invasive treatments, and improve methods for tracking disease progression. As a clinician-scientist, he is dedicated to translating cutting-edge research into practical tools that enhance patient care and streamline clinical decision-making, bridging the gap between technological innovation and clinical application in neurodegenerative disease management.
CONTACT
E: martin.mckeown@ubc.ca
W: https://neurology.med.ubc.ca/faculty-listing/academic/martin-j-mckeown/

Dr Maryam S Mirian
Pacific Parkinson Research Centre and Djavad Mowafaghian Centre for Brain Health, University of British Columbia, Vancouver, Canada
Dr Maryam Mirian is a Research Associate at the Pacific Parkinson Research Centre and the Djavad Mowafaghian Centre for Brain Health at the University of British Columbia. A former Assistant Professor in Electrical and Computer Engineering at the University of Tehran, she holds a PhD in Artificial Intelligence and Robotics. Dr Mirian specialises in developing advanced computational techniques for analysing biomedical signals, including EEG, fMRI, electrodermal activity, and IMU data. Her current research focuses on video-based monitoring of Parkinson’s disease, leveraging computer vision and deep learning to assess motor symptoms such as tremors, bradykinesia, and dyskinesia. Her work aims to extract clinically meaningful insights from multimodal patient data, identifying biomarkers and refining non-linear dynamical models for improved patient stratification, early diagnosis, and personalised treatment strategies.
CONTACT
E: maryam.mirian@ubc.ca
https://www.linkedin.com/in/mmirian/
https://scholar.google.ca/citations?user=7etobUIAAAAJ&hl=en
KEY COLLABORATORS
Jane Z. Wang, PhD. Department of Electrical and Computer Engineering, University of British Columbia
FUNDING
This research was funded by the Pacific Parkinson’s Research Institute and a Collaborative Health Research Project grant from the Canadian Institutes of Health Research (CIHR) in collaboration with the Social Sciences and Humanities Research Council of Canada (SSHRC) and the Natural Sciences and Engineering Research Council of Canada (NSERC).
FURTHER READING
M Gholami, et al., Automatic labeling of Parkinson’s Disease gait videos with weak supervision, Medical Image Analysis, 2023, 89, 102871. DOI: https://doi.org/10.1016/j.media.2023.102871
KW Park, et al., Potential Pitfalls of Remote and Automated Video Assessments of Movements Disorders, Movement Disorders, 2023, 38(3), 504–506. DOI: https://doi.org/10.1002/mds.29325
T Yu, et al., PA-Tran: Learning to Estimate 3D Hand Pose with Partial Annotation, Sensors, 2023, 23(3), 1555. DOI: https://doi.org/10.3390/s2303155
![]()

REPUBLISH OUR ARTICLES
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence (CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
SUBSCRIBE NOW
Follow Us
MORE ARTICLES YOU MAY LIKE

Assoc Prof. Nicholas Brown | Rethinking Prostate Care: A New Frontier in Treating Benign Prostatic Hyperplasia
For millions of men, ageing brings with it a set of frustrating and often disruptive urinary symptoms. These symptoms, caused by benign prostatic hyperplasia, or BPH, can affect sleep, confidence, and overall quality of life. Traditionally, treatment follows a familiar path. Patients begin with medications, often for years, and may eventually progress to surgery if symptoms worsen. Yet this pathway is not without its drawbacks. Medications can cause side effects, while surgery carries risks and recovery time. In recent years, a minimally invasive interventional radiology procedure called prostate artery embolisation, or PAE, has begun to challenge this traditional model. At the forefront of this shift is a collaborative research group, led by Dr. Nicholas Brown of the University of Queensland, whose series of P-EASY studies has explored whether PAE could transform how BPH is treated, particularly at earlier stages.

Jean Lycke | Addressing Unmet Medical Needs in Mucosal Disease: A Close-to-Market Innovation Approach
Recurrent Aphthous Stomatitis (RAS) is an oral condition characterized by one or several painful mucosal ulcers. RAS affects a large proportion of the population and has a point prevalence of approximately 2–3%, daily. The etiology remains unknown, and there is currently no curative treatment. Most patients experience recurring episodes over time, with each episode typically lasting up to a week. Here, we describe the development of a mucoadhesive patch which, when applied over a RAS ulcer, provides rapid pain relief. The patch is easy for patients to apply when symptoms begin and has the potential to be used as an over-the-counter product. The development of the Mucocort mucoadhesive patch is an example of a Close-to-Market innovation strategy that embraces simplicity within a complex healthcare system. By simplifying the product concept, the team has reduced the number of regulatory steps required before market approval. This MedTech/Pharma innovation model, known as the “4R” framework – Re-purposing, Re-formulation, Re-positioning, and Re-patenting – has guided the program from concept to commercialization. In addition to the biodegradable mucoadhesive patch developed for RAS ulcers, the team is extending the innovation concept to a mucoadhesive gel formulation for the prevention and treatment of chemotherapy-induced mucositis. This gel-based program is being commercialized separately through MucoShield.
The Translational Asian Agerelated Macular Degeneration Program Phase 2 (TAAP-2): Reimagining the Future of Vision Care
Age-related macular degeneration, often abbreviated as AMD, is one of the leading causes of vision loss among older adults worldwide. In Asia, where populations are ageing rapidly, its impact is particularly profound. For many, the disease quietly erodes central vision, making everyday activities such as reading, driving, and recognising faces increasingly difficult. Against this backdrop, the Translational Asian Age-related Macular Degeneration Programme, or TAAP for short, has emerged as a bold and ambitious effort to confront the disease headon. Now in its second phase, TAAP-2 represents a significant evolution in both scientific scope and clinical ambition.
Ms. Aikaterini Dritsoula | Looking Beyond Snoring: How Hidden Airway Problems Shape Children’s Sleep
For many parents, a child’s snoring may seem harmless, even endearing. Yet in some cases, it signals something more serious. Obstructive sleep apnoea is a condition in which a child’s breathing is repeatedly disrupted during sleep. These interruptions can affect growth, behaviour, and learning. Children with this condition may toss and turn at night, struggle to concentrate during the day, or show signs of hyperactivity and fatigue. Traditionally, enlarged tonsils and adenoids have been seen as the main culprits. Surgery to remove them has long been considered the standard treatment. However, research led by Consultant ENT Surgeon Ms. Aikaterini Dritsoula of The Leeds Teaching Hospitals NHS Trust invites us to look deeper. Her work suggests that the story is often more complex, especially in very young children.