Effective Treatments from Ancient Practices
Acupuncture is one aspect of Traditional Chinese Medicine (TCM), the practice of which began over two millennia ago. This ancient practice involves the insertion of fine needles into the skin at specific points along the body. These points are known as acupoints, located along pathways called meridians. According to TCM, meridians are routes through the body along which energy, or Qi, flows. Although acupuncture has been practiced for thousands of years, it is only in recent decades that it has been tested from an evidence based approach.
Western medical practitioners have often approached acupuncture with scepticism. There are a number of reasons behind this, including a lack of verification of the underlying concepts such as Qi and meridians, and the overall absence of the scientific method. Clinical trials have produced mixed results and are open to bias and the placebo effect. It should also be noted that around one third of patients do not respond well to treatment.
Upon observing acupuncture in practice for the first time in the early 90s, Dr John Longhurst was similarly sceptical, due to an insufficiency of scientific evidence. ‘I was asked to consider collaborative research in acupuncture. My initial reaction was no, but my future collaborator, Dr Peng Li, then Professor and Chair of the Department of Physiology at Shanghai Medical University, showed me his curriculum vitae containing publications in respected western journals on the central neural mechanisms underlying acupuncture’s cardiovascular actions,’ Dr Longhurst tells us. This led to a long-term collaboration between the two scientists, exploring the neural mechanisms underlying the actions of acupuncture on cardiovascular function. Dr Stephanie Tjen-A-Looi soon joined them, and the team went on to carry out over 40 experimental and clinical studies on the effects of acupuncture on myocardial ischaemia (reduced blood flow to the heart), reflex induced hypertension (high blood pressure), sustained hypertension and reflex hypotension (low blood pressure), as well as identifying mechanisms that underlie the physiological effects of acupuncture.
One of the most significant areas of study in acupuncture has been the role of the nervous system. Multiple studies suggest that meridians are in fact neural pathways along which nerve bundles are located. ‘We have conducted a large number of studies – over 40 in total – showing that electro- and manual acupuncture applied at specific acupuncture points lowers short-term elevations (by about 50%) and long-term elevations in blood pressure through stimulation of sensory nerve fibres underlying the acupuncture points,’ Dr Longhurst explains. A 2005 study by the team showed that the transection (cutting) of sensory nerve fibres eliminated the modulatory effect of acupuncture on cardiovascular responses. They did not observe similar outcomes with eliminating the actions of motor nerve fibres, suggesting an important role for sensory neural pathways in acupuncture.
Acupuncture and Mechanisms of Action
Over the last two decades, many mechanisms of action on cardiovascular function have been identified. These mechanistic studies are significant, as they help to guide clinical studies. The central nervous system (CNS) plays a key role in mediating the physiological responses of the cardiovascular system. Contained within the CNS are centres that regulate the function of autonomic nerves – important regulatory nerves that control different aspects of cardiovascular function such as heart rate, blood pressure, cardiac output and peripheral blood flow.
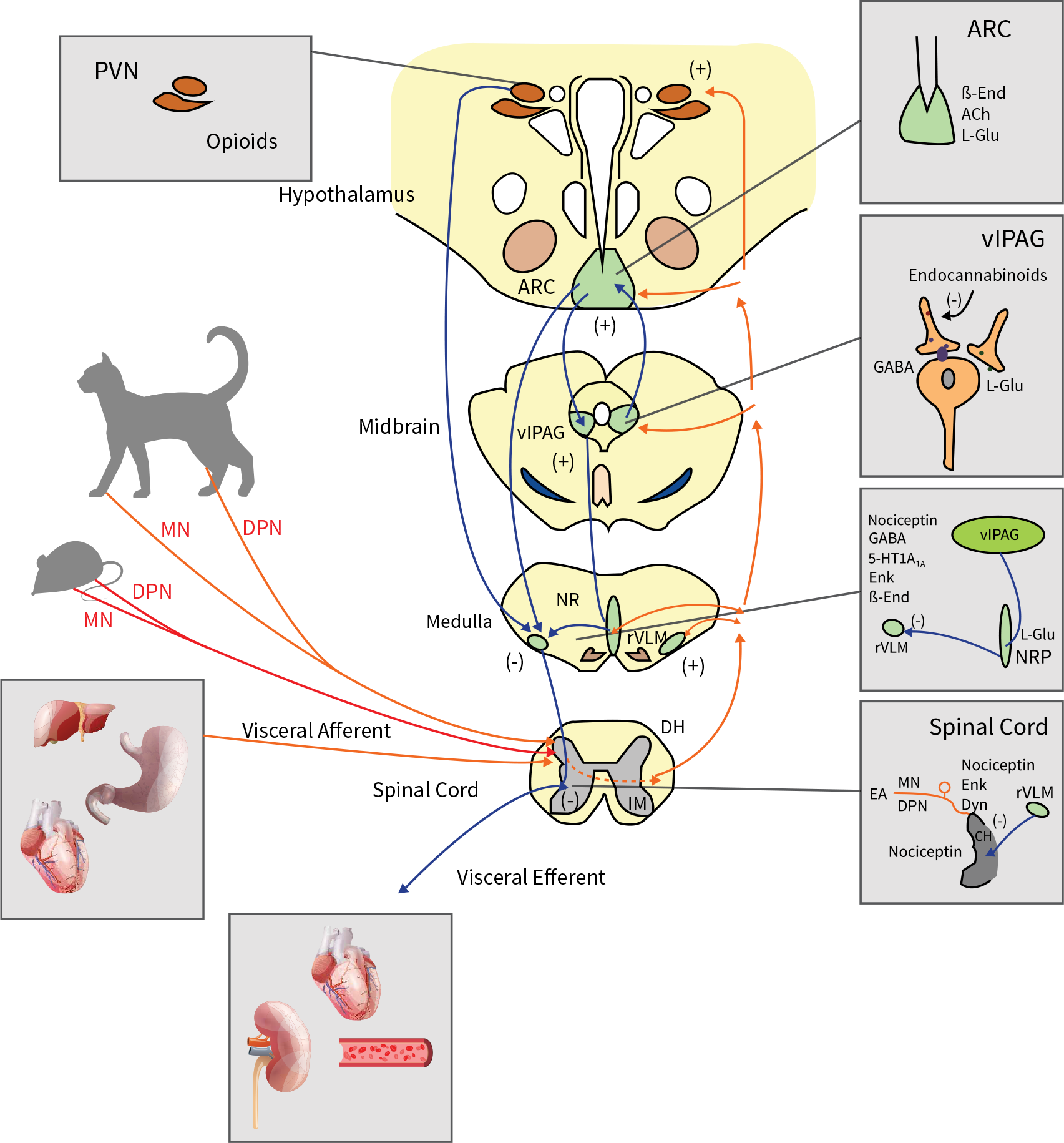
Electroacupuncture’s modulation of reflex increases in blood pressure is based on a long-loop pathway involving at least three areas of the brain: the hypothalamus, midbrain and medulla. These areas are relevant to the autonomic nervous system (which functions to regulate the body’s unconscious actions). The autonomic nervous system can be divided into two branches: the sympathetic nervous system (which stimulates ‘fight or flight’) and the parasympathetic nervous system (which stimulates ‘rest and digest’). Under different conditions acupuncture acts on these two branches of the autonomic nervous system to produce effects on the cardiovascular system.
Several of the relevant neurotransmitter systems involved in these actions are located in the rostral ventrolateral medulla (rVLM), which is responsible for the control of sympathetic outflow associated with cardiovascular function. Electroacupuncture stimulation applied for 15 to 30 minutes activates a long-loop pathway, leading to the oopioid (Beta-endorphin (ß-End) and Enkephalin (Enk)) mediated regulation of rVLM neurons through the inhibition of the excitatory neurotransmitter glutamate (L-Glu). Other neurotransmitter systems in the rVLM (namely GABA released from the rostral and caudal ventrolateral medulla and serotonin released from the nucleus raphé pallidus) also participate in the regulation of hypertension.






{kind=link}