
Professor Heidi Zeeman – Neurophilic Design: Who We Are and Where We Are
Professor Heidi Zeeman of Griffith University and her collaborators are exploring the innovative research field of neurotrauma and the built environment. They endeavour to understand the experiences of individuals with different brain sensitivities and neurological disabilities and the environments in which they live, work and recover. This work will ultimately inform next generation therapeutic environments, workplace and residential design and the design of public spaces.
In modern society, the external environment around us is constantly changing. Similarly, throughout different stages of life, our internal interpretation of and response to our environment also changes – our idea of ‘home’ as a child might differ significantly to the ‘home’ that we depict in our minds as an adult. In essence, our life experiences shape our environment, and yet our environments also shape our life experiences. Considering this, how often are we aware that our experience of the environment may be considerably different than through the eyes of another, perhaps even adversely so?
Demographics predict that an increasing proportion of the population will relocate to urban environments in the coming decades. Individuals with neurological, neurosensory, psychological or psychiatric conditions will represent a large percentage of the general population. The emerging need to recognise how individual differences and neurosensitivities contribute to a person’s interaction with their environment has resulted in an everexpanding research field, which might be termed neurophilic design, broadly relating to the human brain’s unique affiliation with the built environment.
As an extension of a biophilic understanding of the world, where humans possess an inherent affiliation with the natural environment, Professor Zeeman of the Menzies Health Institute Queensland and The Hopkins Centre (https://www.hopkinscentre.edu.au/) describes neurophilic design as reliant on an evolved and complex neurocognitive system comprising reception, perception and association that determines the nature and extent of human interaction with the external environment.
 The neurocognitive environment work of Professor Zeeman is centred on the foundation principles established by Kurt Lewin’s Field theory in 1936 where human behaviour is a function of the person (P) and their environment (E). In a more nuanced way, the Environmental-Press model proposed by M. Powell Lawton suggests that person-related competencies and needs manifest differently in different environments, leading to dissimilar (either stressful or supportive) outcomes or levels of ‘fit’. Accordingly, after neurological injury or illness, individual competencies are likely to alter, and as such, environments must also adapt to the person in order to facilitate recovery and promote optimal engagement with the environment. We are only beginning to understand how best to modify the environment to optimise intraindividual functioning.
The neurocognitive environment work of Professor Zeeman is centred on the foundation principles established by Kurt Lewin’s Field theory in 1936 where human behaviour is a function of the person (P) and their environment (E). In a more nuanced way, the Environmental-Press model proposed by M. Powell Lawton suggests that person-related competencies and needs manifest differently in different environments, leading to dissimilar (either stressful or supportive) outcomes or levels of ‘fit’. Accordingly, after neurological injury or illness, individual competencies are likely to alter, and as such, environments must also adapt to the person in order to facilitate recovery and promote optimal engagement with the environment. We are only beginning to understand how best to modify the environment to optimise intraindividual functioning.
Over the past ten years, Professor Heidi Zeeman and her research team have conducted emergent research in this field, particularly focusing on individuals with neurotrauma such as brain injury and spinal injury. Professor Zeeman says that, ‘we know that environments influence how people think, feel and behave. However, we aren’t clear about the transactional nature of this important relationship. In other words, what influences what, to what degree and how? If we are able to understand the limits of brain function in relation to the environment by studying brain inflammation and extreme injury compared to normal function, then we are more likely to determine what works in terms of environmental enrichment for the general population.’
E-book

Audio-book

Reference
https://doi.org/10.26320/SCIENTIA288
Share
{kind=link}
To achieve this, Professor Zeeman and her colleagues work collaboratively with experts from multiple disciplines and industry sectors. She describes how, ‘our team are involved with medical professionals, engineers, virtual reality developers, environmental psychologists, nursing, allied health practitioners, architects, economists, artists, urban planners and neuroscientists to explore human sensitivity to the built environment.’
A Neurocognitive Approach (NEUROCODE©) to Placemaking
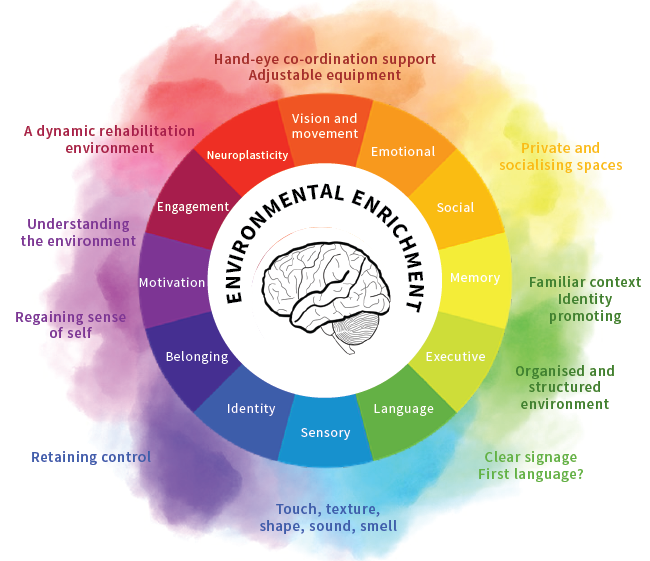
For individuals who are neurodiverse, neurosensitive, and for those who experience brain change due to ageing, injury or illness, environments can be either supportive or stressful to the human condition. Building on the neuropsychological framework of the human brain and behaviour, the neurocognitive design (NEUROCODE©) approach under development by Professor Zeeman and her team proposes a ‘whole-of-brain’ design system, where core aspects of brain function are mapped to specific evidence-based environment modules. Both typical and atypical brain function is addressed, allowing for a more personalised and inclusive approach to built environment design.
Intended to be used by health and design professionals, a comprehensive neurocognitive system will provide much-needed insight into how environments can optimise human performance and bring together a diverse scientific nomenclature. For instance, the approach seeks to identify evidence-based design elements that have been shown to be helpful for health settings (covering sensory features), as well as those design elements that may be unintentionally harmful for people with specific brain conditions, such as post-traumatic stress disorder, schizophrenia, dementia, autism, and traumatic brain injury.
Residential Environments for Individuals with Neurological Disability
Individuals who have a complex neurological condition, for example, a brain or spinal injury, may require high levels of health support on a daily basis, yet they are eager to regain their independence as quickly as possible. However, a lack of understanding as to how the immediate environment (such as home, transport systems and workplaces) must be specifically influenced and designed to meet the requirements of such individuals has significantly limited the residential and community-based options available to them.
As part of her PhD research, Dr Courtney Wright (supervised by Professor Zeeman) conducted a comprehensive systematic review that aimed to clarify the broader factors relating to residential needs and design solutions for this population. The review covers 26 studies in which 198 unique housing features were identified. Of the 198 features, 142 relate to the design of the house, 12 relate to the location and 54 relate to the surrounding neighbourhood (see further reading for more information).
Dr Wright examined the question, ‘what housing features reported in the literature ought to (or should not) inform housing development and design for adults with a neurological disability?’ With an industry partner, Youngcare, Dr Wright has subsequently developed an online tool from her PhD work, to assist people with disability and their family to think about the needs of their residential setting, and better identify components that would be most important.
A Cross-sectoral Approach to Inclusive Housing Development
The residential inclusion of people who require high health and support needs has traditionally been neglected in the mainstream housing market. Professor Zeeman says that people with complex disabilities ‘can be at risk of either high housing mobility (cyclical patterns of temporary accommodation) or housing immobility (trapped in residential aged care homes with little option to move), and few housing solutions are just right.’
To address this problem and attract the necessary broadbased investment required to meet supply and demand, the involvement of the private housing and construction sectors is essential. However, significant commercial entities in Australia who are well-positioned to deliver cost-effective, adaptable and well-designed disability housing remain largely uncertain of the disability market, related policy frameworks, and are unclear about what end-users want and consider to be important in terms of housing design.
To ensure that housing investment is not squandered, it is critical to make timely, cross-sectoral and integrated decisions that maximise outcomes for Australians with complex disabilities. In the context of public-private partnerships, consumer preferences must be understood and mapped against the priorities of other stakeholders. Professor Zeeman and her team employed a systematic method of analytical hierarchical processing (AHP) to assess, and prioritise, seemingly competitive choices within the multi-faceted supported housing sector to ultimately improve quality of life and housing outcomes for people with a disability.
A three-year Australian Research Council project, led by Professor Zeeman, Professor Elizabeth Kendall and Dr Ali Lakhani, and co-funded by the Motor Accident Insurance Commission (Qld), identified a set of consumer-led housing priorities, and 16 sub-areas for inclusive housing development and planning. After consulting with end-users, and professionals from the housing design, construction and health sectors, the team identified four core decision areas critical in developing inclusive housing.
End-user connectedness was prioritised above all other decision points by both consumers and professionals, followed by feasibility priorities, design priorities and build priorities. Within end-user connectedness, the subset of consumer-based priorities (in ranked order) included access to health services, community engagement, proximity to transport, safety, security and transport. Each of the remaining core decision areas was further defined by a distinct subset of priorities. The research received an Innovation Award at the 15th International Symposium on AHP in Hong Kong, July 2018, and an industry decision support resource is currently under development.
This work of Professor Zeeman and her team extends the current understanding of suitable housing for individuals with neurological impairments. Their research also provides the opportunity for future inclusive housing provisions to adopt the key features identified by the team, to create a positive environment for people with neurological conditions.

Hospital Rehabilitation Environments
Professor Zeeman and her PhD graduate, Dr Jacinta Colley, have also invested a considerable amount of time into discovering the optimal neurorehabilitation inpatient environment following a brain or spinal cord injury. Over the course of three years, Dr Colley and key stakeholders from a neurorehabilitation hospital (including patients and staff) identified that inpatient rehabilitation facilities represent a mid-point between the hospital and the home. As such, they must support two key environment-person processes – change and certainty. Importantly, Dr Colley identified that if these environments are tailored to the individual’s own neurological impairment and recovery journey, there is a better chance that a more positive recovery outcome will be achieved.
Specifically, when considering change, a neurorehabilitation environment should be dynamic in that it promotes individual improvement and development of independence over time. This is based on the concept that the varying levels of care that come with recovery from a brain injury require different environments at each stage, thus encouraging a natural transition into an independent environment.
With regards to certainty, neurorehabilitation also needs to place emphasis on an individual’s own understanding of their environment, how it contributes to their regaining a sense of self and how it contributes to their sense of regaining control. Dr Colley and her colleagues suggest that by supporting these two key processes, the necessary pathway for promoting human engagement with the environment will be achieved.
In related work, Professor Zeeman is collaborating with project lead, Professor Julie Bernhardt of the Florey Neuroscience Institute, to develop an optimised virtual environment living lab for stroke. Evidence-based architecture is a growing field of research that will ultimately inform better rehabilitation facility design. Adopting a design science approach, this project will incorporate experiences from stroke patients, together with insights of key stakeholders representing hospital architecture and technology to model a variety of innovative designs that optimise the recovery and rehabilitation process.
Designing for the Future
Professor Zeeman says the next steps for her team are, ‘to focus on experimental analysis of the brain and environment and to explore the parameters of brain plasticity to identify opportunities for precision environments, and sensory and spatial design, in order to optimise person-place interactions.’ She adds that, ‘we have developed, evaluated and influenced neurorehabilitation environments and services, developed conceptual models based on evidence, and we have facilitated and maintained important industry research partnerships to deliver better environments, services and support for people who are vulnerable and are in difficult times in their life.’
Nonetheless, she states, ‘this is an exciting time in neuroplasticity research. Enriched environments have so much to offer people with neurosensitivity and diversity. We have the skills and tools now to better determine the impact and evidence, which have eluded us for so long. For instance, my colleague, Dr Ali Lakhani, is doing fantastic work using virtual reality to alleviate neuropathic pain after spinal cord injury, and applying geographical information systems to map disability services and environments to better inform urban planning.’
Failing to incorporate a broader understanding of inclusive design poses a threat to the long-term biological and psychosocial health and wellbeing of people with neurodiversity, young people with disability and our senior citizens. It is therefore imperative that the work of Professor Zeeman and her team continues to be applied in real-life contexts.
Meet the researcher

Professor Heidi Zeeman
Menzies Health Institute Queensland
Griffith University
Brisbane, Queensland
Australia
Professor Heidi Zeeman is a Principal Research Fellow at the Menzies Health Institute Queensland and The Hopkins Centre, Griffith University. She completed a PhD in 2007 and began her research career at the Centre of National Research on Disability and Rehabilitation Medicine (CONROD). Professor Zeeman conducts research into human health and the built environment, in collaboration with the health, disability, urban planning, arts and construction sectors. A key focus of her work is to understand the experiences of individuals that have experienced neurotrauma within the environments in which they live, work and recover. She has completed multi-year evaluations of major public health programs and health facilities in Australia over the past decade, novel workforce training programs, predictive models of health, and guidelines for practice. Professor Zeeman is widely published in international journals and has been awarded multiple prestigious awards over her 17-year academic career, including a number of Australian Research Council grants, post-doctoral fellowships, a Fulbright Scholarship (2014) and a Churchill Scholarship (2009).
CONTACT
E: h.zeeman@griffith.edu.au
W: https://experts.griffith.edu.au/academic/h.zeeman
FURTHER READING
CJ Wright, H Zeeman, E Kendall, and JA Whitty, What housing features should inform the development of housing solutions for adults with complex physical and cognitive disability?: A systematic review of the literature, Health & Place, 2017, 46, 234V248.
J Colley, H Zeeman and E Kendall, Everything happens in the hallways: Exploring user activity in the corridors at two rehabilitation units, Health Environments Research and Design Journal, 2017, 1–14.
H Zeeman, E Kendall, J Whitty, CJ Wright, C Townsend, D Smith, A Lakhani and S Kennerley, Study protocol: Developing a decision system for inclusive housing: Applying a systematic, mixed-method quasi-experimental design, BMC Public Health, 2016, 16, 261.
H Zeeman, Places, communities, and cultures: Drawing on the strength of many, In Health and Healing after Traumatic Brain Injury: Understanding the Power of Family, Friends, Community and Other Support Systems, United States: Praeger, 2013, 187–188.
H Zeeman, C Ehrlich, E Kendall and M Vit, Experience of place for young adults under 65 years with complex disabilities moving into purpose-built residential care, Social Science & Medicine, 2012, 75, 2151–2159.
D Smith, C Wright, A Lakhani and H Zeeman, Art processes: A research tool for acquired brain injury and residential design, Arts and Health, 2017, 9, 251–268.
![]()