
Dr Stephen Kry – Improving the Quality and Accuracy of Radiotherapy Through Research
{kind=link}
Radiation therapy is an effective and widely used method of treating cancer, and as with any treatment, it is essential to get the right dose. However, Dr Stephen Kry from The University of Texas MD Anderson Cancer Center has found widespread errors in the systems that calculate the doses patients receive. Through his research, he has helped to identify where these errors occur, how common they are, and provide possible solutions. He hopes that his work will go on to improve the quality and efficacy of radiotherapy for many cancer patients.
Cancer Prevalence and Treatments
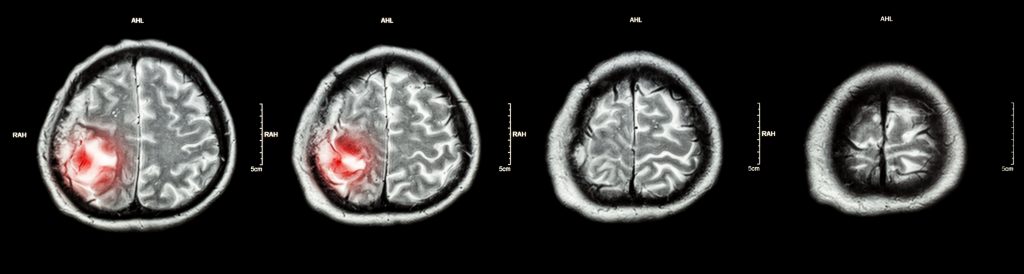
Cancer is a disease that touches almost everyone in some way, at some point in their lives. In fact, half of all people will develop it. Characterised by the overproduction of cells in a specific part of the body, some cancers have the ability to cause destruction where they grow and spread to other tissues. As the human body has over 200 types of cells, there are over 200 types of cancer, but among the most common are those occurring in the head and neck, breast, prostate, lung and bowel.
Thankfully, cancer research has made incredible progress over the last few decades and many types of cancer now have effective treatments. If the cancer has produced a solid tumour, surgery is often the first step to begin fighting back. Some patients receive chemotherapy, which targets cells that multiply more often than the body’s normal cells. Because chemotherapy drugs are circulated through the bloodstream, they can reach cancer cells in most parts of the body. Other patients may instead, or in addition, receive radiotherapy.

Radiotherapy: Is It safe, Is It Effective?
About 50% of people with cancer receive radiotherapy as part of their treatment. This may be with the aim to eradicate the cancer, make a tumour smaller to facilitate its removal (called neoadjuvant treatment), or just to relieve and control symptoms.
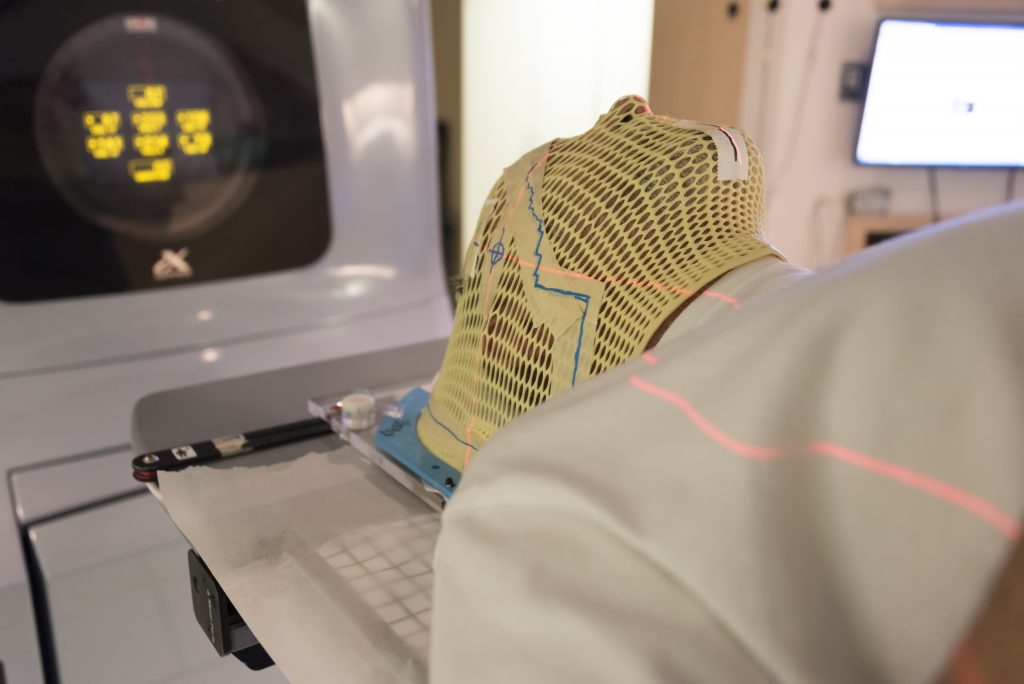
Most often this is done as external radiotherapy, where a machine known as a linear accelerator is used to direct ionising radiation or high-energy electromagnetic waves (i.e., X-rays) at a tumour. Internal radiotherapy involves swallowing or injecting a radioactive liquid or inserting a radioactive object near cancerous cells. The radiation from both procedures creates damage to the DNA within the cells, which prevents them from growing and dividing. Eventually, if the treatment is successful, the cancer cells die and the tumour stops growing. It is important that a sufficient dose of radiation is delivered to kill the tumour. Healthy cells around the tumour can also be damaged by radiotherapy, but they usually recover after some time.
Like all cancer therapies, radiotherapy has side effects, and too much radiation dose increases the risk and severity of these side effects. Two of the most common consequences are general fatigue in the following weeks and sore and red skin where the radiation had been targeted. Depending on where the patient has been treated, they may also experience decreased salivary production (dry mouth) for patients treated in the head and neck, shortness of breath for patients treated in the lung, or diarrhoea or rectal bleeding for patients treated in the pelvis. If the goal is to cure the cancer, not just lessen symptoms, radiotherapy is often given five days a week for one to seven weeks. The result is that 40% of people who receive radiotherapy as part of their treatment are cured.
External radiation therapy, in particular, is very technologically complex. There are more than 100 simultaneously moving parts on a linear accelerator shaping the radiation dose in three dimensions to ensure the radiation is limited, as much as possible, to just the tumour. This complex delivered dose must accurately match the intended dose, which is calculated in 3D using specialised computer systems. It is necessary that the intended and delivered dose agree to ensure that the patient has received the optimal dose. Disagreements could lead to not enough dose being delivered and a reduced chance of killing the tumour, or too much dose being delivered and excess side effects.
Phantom Heads
The term ‘head and neck phantom’ may conjure up images more in line with Halloween than cancer research. However, they are in fact a vital part of Dr Stephen Kry’s studies into radiation oncology at The MD Anderson Cancer Centre. Head and neck phantoms are anatomically realistic models of a human head. Their shape, proportions and density mirror the real thing and inserts include simulated tumours as well as organs at risk. Devices called dosimeters within the phantoms measure the amount of radiation a specific location in the head has received. Using these phantoms, the accuracy of radiation therapy can be tested.
This phantom was developed by the Imaging and Radiation Oncology Core (IROC) in 2001. IROC provides quality assurance support for clinical trials by the USA’s National Cancer Institute, ensuring that all institutions provide consistent and accurate radiotherapy doses. IROC monitors more than 2,000 radiotherapy clinics and hospitals worldwide, and the head and neck phantom is irradiated by around 200 institutions every year.
Finding the Errors in Radiotherapy Delivery
While this phantom was originally developed to credential institutions who wish to partake in clinical trials, it is also broadly used by institutions who want to assure themselves that they are able to deliver radiotherapy correctly. The phantom tests the simple but critical objective of whether the institution can deliver the dose they intend to deliver. This practice has a number of benefits as it not only reduces variability across the studies but it also helps institutions identify errors within their own processes and make improvements for the future.
To pass, institutions have to give the head and neck phantom a delivered dose within 7% of what was planned, within 4 mm of the planned spot. These criteria are loose compared to the dose accuracy needed biologically and compared to what should be achievable technically – institutions should be able to deliver the dose within 2–3%. When this testing started in 2001, pass rates started at 66%. Although they are now around 90%, this is still not quite good enough for Dr Kry, given that it means ~10% of institutions still fail to deliver radiation doses that are appropriately accurate. There were no studies that investigated the reasons why this was happening until recently, when Dr Kry and his team set out to find answers.
Using a thermoluminescent dosimeter, they determined the accuracy of radiation delivery on head and neck phantoms across hundreds of institutions. The team found that most failures to pass the phantom test were due to incorrect doses being delivered – usually too little radiation. Small inaccuracies and errors in the institution’s configuration of the dose calculation software were identified as primary culprits.
Dr Kry and his colleagues were concerned about the high levels of inaccurate radiation dose delivery across the sites IROC worked with. This issue could directly and negatively affect cancer patients: unexpectedly under-dosing patients may lessen their risk of side effects, but it would also lessen the chance that their cancer was cured. Dr Kry saw that resolving inaccuracy was of the utmost importance. To resolve these dose discrepancies, it was necessary to understand where errors were originating from so that institutions could address these issues.
Revealing Dose Errors
Dr Kry investigated several aspects of the way in which institutions predict radiation dose using their specialised computer system. Because the radiation delivery is so complex, the computer system is customised at each institution to describe each unique radiation beam. This process of modelling the physical radiation beam within the computer system is a complex process with ample opportunities for errors.
The first evaluation was of basic characteristics and calculations from the computer. IROC compared measured and delivered doses for more than 1,000 radiation machines at institutions that participated heavily in clinical trials. The institutions selected for evaluation focussed on those that involved higher numbers of patients in clinical trials. These establishments usually had no particular concerns about their dosing. A focus of these visits was to evaluate radiation dosimetry – how well the dose calculated by the treatment planning system matched that actually given. This was done for simple radiation fields (e.g., a square beam of radiation, instead of a complex-shaped field that would be used to treat a patient).
The team discovered that even for these simple cases, dosing inaccuracies were relatively common and came down to errors in how the institution had modelled the radiation in their computer system.
For more complex and realistic patient treatments, Dr Kry dug further into the head and neck phantom program. Dr Kry and his team developed a system to recalculate 259 head and neck phantom irradiations to search for and identify calculation errors in institutions’ treatment planning systems. Using this system, the team evaluated the doses to the head and neck phantom that were predicted by hundreds of cancer centers, each using their own clinical treatment planning system. Dr Kry’s team found a concerning number of failures in the ability of institutions to calculated doses accurately. If an institution had failed the head and neck phantom test originally, the team revealed that 68% of them were due to calculation inaccuracies. Overall, a concerning one in five institutions showed errors in their treatment planning systems for radiotherapy
Using this new evaluation system, Dr Kry and his colleagues can now inform an organisation when their treatment planning system is inaccurate. They want to emphasise the importance of creating accurate beam models in the treatment planning system so that patients are given the best possible care.
To aid institutions in improving the accuracy of their treatment planning system calculations, Dr Kry’s team has worked on providing guidance on how to better develop beam models. For example, in 2019, they created a dataset that could be used as a reference by people testing their treatment planning systems. This helps them to assign the correct parameter values to the systems so that the consequent beam models calculate the correct radiation dose for the patient. Enabling an institution to double-check their calculations and detect anomalies in this way allows them to confidently treat their patients, knowing the dose they are giving is as accurate as possible.

Head and neck phantom. Credit Stephen Kry
Work for the Future
Dr Kry hopes that his team’s research will aid the continuing improvement of the quality and accuracy of radiation therapy. He has identified the magnitude and origin of dosing errors that are unfortunately common in radiation oncology. Based on the underlying causes of dosing errors, he has developed practical solutions that can be used in real-world treatment centres. As clinical physics develops and evolves, his work will undoubtedly be useful for a long time to come.
Reference
https://doi.org/10.33548/SCIENTIA744
Meet the researcher

Dr Stephen Kry
MD Anderson Cancer Center
The University of Texas
Houston, TX
USA
Dr Stephen Kry hails from Calgary, Canada. He completed his Bachelor of Science (Honours) in Physics in 1999 at the University of British Columbia in Vancouver. He then went on to receive both his MSc in Medical Physics and his PhD in Medical Physics from The University of Texas MD Anderson Cancer Center in Houston. Whilst taking on many appointments and responsibilities throughout the years as part of various professional and scientific societies, he has also fulfilled numerous roles at MD Anderson. Currently, Dr Kry is a tenured Associate Professor in the Department of Radiation physics. He is the director of MD Anderson’s Accredited Dosimetry Calibration Laboratory, Principal Investigator of the Imaging and Radiation Oncology Core (IROC), and Director of the Houston office of IROC. He is a member of the Graduate School of Biomedical Sciences at The University of Texas Health Science Center where he maintains a laboratory with several graduate students. His work has earned him multiple honours and awards such as the Highest Commendation from the Graduate School of Biomedical Sciences at his university. Dr Kry’s research focuses on improving the safety and quality of radiotherapy treatments for cancer patients.
Contact
E: skfry@mdanderson.org
W: https://faculty.mdanderson.org/profiles/stephen_kry.html
Funding
National Cancer Institute
Further Reading
SS Edward, PE Alvarez, PA Taylor, et al., Differences in the patterns of failure between IROC lung and spine phantom irradiations, Practical Radiation Oncology, 2020, 10(5), 372–381.
MC Glenn, CB Peterson, DS Followill, et al., Reference dataset of users’ photon beam modeling parameters for the Eclipse, Pinnacle, and RayStation treatment planning systems, Medical Physics, 2020, 47, 282–288, doi:10.1002/mp.13892
MC Glenn, CB Peterson, RM Howell, et al., Sensitivity of IROC phantom performance to radiotherapy treatment planning system beam modeling parameters based on community-driven data, Medical Physics, 2020, 47(10), 5250–5259, doi:10.1002/mp.14396
SF Kry, L Dromgoole, P Alvarez, et al., Radiation Therapy Deficiencies Identified During On-Site Dosimetry Visits by the Imaging and Radiation Oncology Core Houston Quality Assurance Center, International Journal of Radiation Oncology, Biology, Physics, 2017, 99, 1094–1100.
JR Kerns, FS Stingo, DS Followill, et al., Treatment Planning System Calculation Errors Are Present in Most Imaging and Radiation Oncology Core-Houston Phantom Failures, International Journal of Radiation Oncology, Biology, Physics, 2017, 98, 1197–1203.
ME Carson, A Molineu, PA Taylor, et al., Examining credentialing criteria and poor performance indicators for IROC Houston’s anthropomorphic head and neck phantom, Medical Physics, 2016, 43, 6491.
![]()
Want to republish our articles?
We encourage all formats of sharing and republishing of our articles. Whether you want to host on your website, publication or blog, we welcome this. Find out more
Creative Commons Licence
(CC BY 4.0)
This work is licensed under a Creative Commons Attribution 4.0 International License. 
What does this mean?
Share: You can copy and redistribute the material in any medium or format
Adapt: You can change, and build upon the material for any purpose, even commercially.
Credit: You must give appropriate credit, provide a link to the license, and indicate if changes were made.
More articles you may like
Dr Rhett Martin | Governing Nature at the Edge of Collapse
For millions of men, ageing brings with it a set of frustrating and often disruptive urinary symptoms. These symptoms, caused by benign prostatic hyperplasia, or BPH, can affect sleep, confidence, and overall quality of life. Traditionally, treatment follows a familiar path. Patients begin with medications, often for years, and may eventually progress to surgery if symptoms worsen. Yet this pathway is not without its drawbacks. Medications can cause side effects, while surgery carries risks and recovery time. In recent years, a minimally invasive interventional radiology procedure called prostate artery embolisation, or PAE, has begun to challenge this traditional model. At the forefront of this shift is a collaborative research group, led by Dr. Nicholas Brown of the University of Queensland, whose series of P-EASY studies has explored whether PAE could transform how BPH is treated, particularly at earlier stages.

Assoc Prof. Nicholas Brown | Rethinking Prostate Care: A New Frontier in Treating Benign Prostatic Hyperplasia
For millions of men, ageing brings with it a set of frustrating and often disruptive urinary symptoms. These symptoms, caused by benign prostatic hyperplasia, or BPH, can affect sleep, confidence, and overall quality of life. Traditionally, treatment follows a familiar path. Patients begin with medications, often for years, and may eventually progress to surgery if symptoms worsen. Yet this pathway is not without its drawbacks. Medications can cause side effects, while surgery carries risks and recovery time. In recent years, a minimally invasive interventional radiology procedure called prostate artery embolisation, or PAE, has begun to challenge this traditional model. At the forefront of this shift is a collaborative research group, led by Dr. Nicholas Brown of the University of Queensland, whose series of P-EASY studies has explored whether PAE could transform how BPH is treated, particularly at earlier stages.

Jean Lycke | Addressing Unmet Medical Needs in Mucosal Disease: A Close-to-Market Innovation Approach
Recurrent Aphthous Stomatitis (RAS) is an oral condition characterized by one or several painful mucosal ulcers. RAS affects a large proportion of the population and has a point prevalence of approximately 2–3%, daily. The etiology remains unknown, and there is currently no curative treatment. Most patients experience recurring episodes over time, with each episode typically lasting up to a week. Here, we describe the development of a mucoadhesive patch which, when applied over a RAS ulcer, provides rapid pain relief. The patch is easy for patients to apply when symptoms begin and has the potential to be used as an over-the-counter product. The development of the Mucocort mucoadhesive patch is an example of a Close-to-Market innovation strategy that embraces simplicity within a complex healthcare system. By simplifying the product concept, the team has reduced the number of regulatory steps required before market approval. This MedTech/Pharma innovation model, known as the “4R” framework – Re-purposing, Re-formulation, Re-positioning, and Re-patenting – has guided the program from concept to commercialization. In addition to the biodegradable mucoadhesive patch developed for RAS ulcers, the team is extending the innovation concept to a mucoadhesive gel formulation for the prevention and treatment of chemotherapy-induced mucositis. This gel-based program is being commercialized separately through MucoShield.
The Translational Asian Agerelated Macular Degeneration Program Phase 2 (TAAP-2): Reimagining the Future of Vision Care
Age-related macular degeneration, often abbreviated as AMD, is one of the leading causes of vision loss among older adults worldwide. In Asia, where populations are ageing rapidly, its impact is particularly profound. For many, the disease quietly erodes central vision, making everyday activities such as reading, driving, and recognising faces increasingly difficult. Against this backdrop, the Translational Asian Age-related Macular Degeneration Programme, or TAAP for short, has emerged as a bold and ambitious effort to confront the disease headon. Now in its second phase, TAAP-2 represents a significant evolution in both scientific scope and clinical ambition.